


Viral bronchiolitis is the most common reason for infants to be admitted to hospital,1,2 yet we seem powerless to do much about it. Physicians who have been in practice for 30 years or more have ridden the rollercoaster of optimism following the publication of randomized controlled trials (RCTs) on bronchiolitis showing the efficacy of bronchodilators, steroids, hypertonic saline and so on, only to have that optimism crushed by subsequent trials with negative results. How is it possible that, as admission rates for bronchiolitis have tripled over the last three decades,3 research has produced only conflicting results leading to the conclusion that nothing works? It seems unlikely that we have simply failed (so far) to find the right treatment and just need to keep looking. Perhaps we are doing something fundamentally wrong.
Where are we now?
Both the Canadian Paediatric Society (CPS) and the American Academy of Pediatrics (AAP) have recently published new guidelines for the diagnosis and management of viral bronchiolitis in infants.1,2 These extensive documents, building on the very welcome inaugural AAP guidelines released in 2006,3 can be summarized as follows: bronchiolitis is a very common illness without treatment options other than supportive care and, perhaps (based on “weak” evidence), inhaled hypertonic saline for inpatients only. In the previous AAP guideline,3 we were advised to consider a trial of bronchodilator in these obviously wheezing infants, but now even this solitary option has been withdrawn owing to lack of efficacy. Therefore, when an infant with bronchiolitis presents to the emergency department with respiratory distress, the number of recommended options for active treatment is officially zero.
Have we been studying the wrong infants?
Pathologically, bronchiolitis simply means inflammation of the bronchioles and can occur in all age groups for a myriad of reasons. In infants, the term has become synonymous with seasonal viral-triggered wheezing. Guidelines on bronchiolitis are based on exhaustive reviews of high-quality RCTs, and the first step in any of these studies is to decide who has bronchiolitis. Remarkably, however, there is no universally accepted definition of viral bronchiolitis in infants. The CPS guideline defines bronchiolitis as “a viral lower respiratory tract infection characterized by obstruction of small airways caused by acute inflammation, edema and necrosis of the epithelial cells lining the small airways as well as increased mucus production” that “typically presents with a first episode of wheezing before the age of 12 months,” although the authors state the guideline is intended for children aged up to 24 months.1 The AAP guideline tells us that bronchiolitis is “a constellation of clinical signs and symptoms occurring in children younger than two years, including a viral upper respiratory tract prodrome followed by increased respiratory effort and wheezing,” but children with recurrent wheezing are excluded.2 Although respiratory syncytial virus is the most common etiologic agent, many different viruses (almost universally sampled from the upper airway only) are responsible for clinically identical lower airway obstruction.1,2 Unfortunately, it remains unclear if these viruses in the upper respiratory tract routinely infect the bronchioles or simply trigger inflammation in the lower airways, or both. Unlike the North American guidelines, a UK guideline defines bronchiolitis by the predominance of crackles rather than wheezes to distinguish it from asthma.4
The point of commonality in these definitions is that only the first episode of viral-triggered wheezing under age two years is labelled as bronchiolitis. If clinically identical wheezing episodes recur after this period, we call it preschool asthma (with treatment recommendations almost opposite to those for bronchiolitis), or, if we are uncomfortable with that label, we tend to rely on terms not found in guidelines, such as reactive airways disease and wheezy bronchitis.5 This rather arbitrary distinction has made its way to most bronchiolitis clinical trials, which restrict enrolment to infants with their first episode of viral wheezing only (Table 1). As discussed below, it remains unclear whether this is justified or can even be accomplished.
Characteristics of Cochrane Library meta-analyses of treatments for viral bronchiolitis
The determination of whether a wheezing infant has ever wheezed before will often depend on parental recall as well as agreement between parent and physician about what wheezing is. Parents, however, are poor at recognizing wheezing in their own children9,10 and will often confuse wheezing with multiple other respiratory sounds.11 Unfortunately, even physicians can be inconsistent at recognizing wheezing.12 The profound consequence is that up to 80%13 of infants who present to the emergency department with signs and symptoms consistent with bronchiolitis as defined by the CPS or AAP guidelines will be excluded from RCTs on bronchiolitis solely because of a history of wheezing as determined by questionable parental and physician recognition and recall of a highly variable clinical sign. Nevertheless, restricting the definition of bronchiolitis to “the first episode of wheezing in an infant” remains the dominant inclusion criterion in published studies (Table 1). Has this well-intentioned but badly flawed clinical definition, rejected by 75% of physicians in a recent British survey,14 led to a sampling error that has unintentionally fueled the litany of contradictory clinical trials driving our national guidelines?
Isn’t this just asthma?
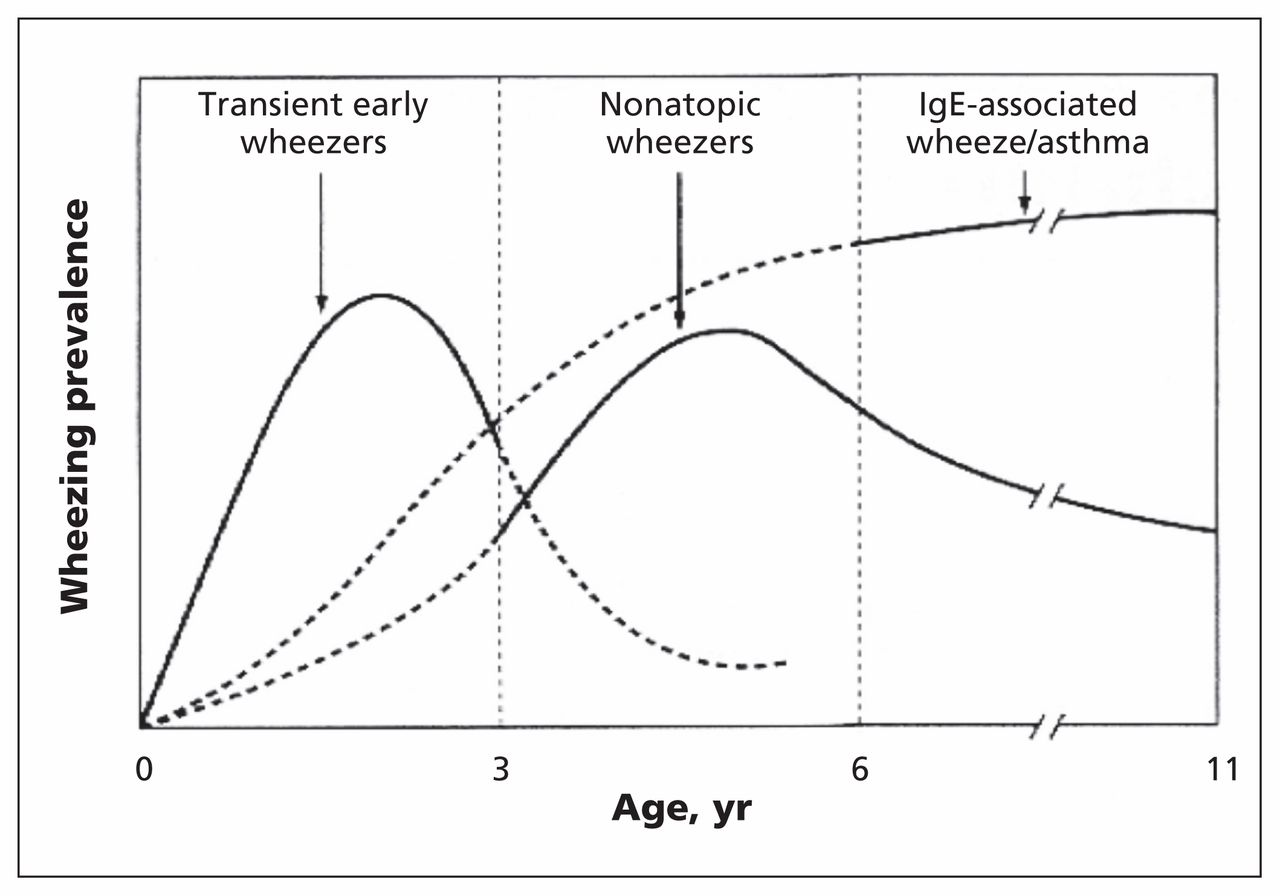
The last decade has given us a much better understanding of asthma in preschoolers — an age group that outnumbers all others in both admissions and emergency visits.15 A 2015 joint position paper of the CPS and Canadian Thoracic Society concluded that asthma can be diagnosed in children one to five years of age, and suspected in children under one year of age, if they have two or more episodes of wheezing and at least some evidence (including only parental report) of response to bronchodilator or steroids.5 If we accept that it is difficult to confirm whether an episode of wheezing is the first or recurrent (as discussed in the previous section) and that many infants with “bronchiolitis” seem to benefit from asthma medications (see next section), we can see there is considerable overlap between this definition of preschool asthma and the CPS and AAP definitions of bronchiolitis. In fact, distinguishing infants with their first and only episode of viral wheezing from those with their first of many subsequent episodes of viral-triggered asthma has been described as “practically impossible.”16 Complicating matters further is the recognition that most exacerbations of preschool asthma are triggered by the same viruses implicated in bronchiolitis.17 Thankfully, the recognition of different wheezing phenotypes in childhood (Figure 1), based largely on age at presentation and the presence of various risk factors, has been instrumental in providing insight into the heterogeneity of preschool asthma. These well-established but imperfect wheezing phenotypes already explain how episodic viral-triggered wheezing in infants fits into the overall pattern of childhood asthma without the need to resort to the arbitrary and unhelpful subtype of bronchiolitis.

Wheezing phenotypes in childhood. Reproduced, with permission, from Stein and colleagues.18 Note: IgE = immunoglobulin E.
Historically, several pathophysiologic differences have been described that may distinguish bronchiolitis from viral-triggered asthma, with the most fundamental being that perhaps only in bronchiolitis does the viral infection appear to extend from the upper to the lower respiratory tract.17,19 Nevertheless, these descriptions also overlap and are based on past studies influenced by the same sampling error mentioned earlier. In addition, is it more reasonable to point to these differences as evidence of two distinct illnesses with very different treatment guidelines (as we have done in the past) or to accept that perhaps bronchiolitis is simply what viral-triggered asthma looks like in infants? After all, we know that the lungs of infants are more prone to small airway occlusion and atelectasis during upper or lower respiratory tract infections compared with older children.19 We also know that the immune system matures with age, leading to qualitative differences between infants and older children in the way they respond to viral infections and allergic triggers.17 Infants are not simply small toddlers, and it is reasonable to expect there to be age-related differences in the histologic appearance of airways in patients with viral-triggered asthma, but does this justify labelling them as distinctly different diseases?
But if it’s asthma, then why don’t asthma medications work?
Our acceptance that bronchiolitis is distinct from asthma may have been nurtured by the observation that the medications so effective in wheezing older children (with asthma) don’t seem to work as well in wheezing infants (with “bronchiolitis”). The most logical explanation, as mentioned in the previous section, is that viral-triggered inflammation leads to airway narrowing in older children but leads to more difficult-to-treat occlusion and atelectasis in infants. Despite this anatomic disadvantage, asthma medications still appear to work more than occasionally in infants. If, for convenience, we consider only the most recent in the series of Cochrane Library meta-analyses examining the role of asthma therapies in bronchiolitis, there are two important observations (Table 1). First, the cumulative evidence suggests that steroids and bronchodilators, the cornerstones of asthma therapy, do not work in infants with bronchiolitis. Second, about a third of these RCTs, all selected for methodologic strength, reached dissenting conclusions.
Focusing on the use of bronchodilators, easily the most controversial and extensively studied treatment, the 2014 Cochrane review6 examined many outcome measures and reaffirmed previous conclusions that bronchodilators are ineffective in bronchiolitis, but at least 12 of the 31 included studies concluded that bronchodilators were effective. Considering only respiratory distress scores, 64% of infants benefited from bronchodilators, but the improvement in scores, although statistically significant, was small and judged to be not clinically significant.6 It is critical to note, however, that these studies compared nebulized bronchodilator coadministered with 0.9% normal saline and “placebo” containing only nebulized normal saline. In a reappraisal of an earlier Cochrane Review of this topic, it was noted that inhalation with normal saline alone successfully reduced respiratory distress scores in 43% of infants in the control arms.20 We already know that inhaled 3% hypertonic saline improves airway clearance in bronchiolitis8 and that perhaps it is the total amount of sodium chloride delivered to the airway surface, and not the concentration nebulized, that is beneficial.21,22 It is therefore not surprising that inhalation of normal saline appears to be beneficial in bronchiolitis.13,20,22,23 Thus, the past unintentional use of an active therapeutic agent as placebo calls into question current conclusions that bronchodilators are not helpful in wheezing infants. Clinicians seem to share this skepticism, and most24 continue to use bronchodilators (almost universally nebulized with normal saline) in bronchiolitis despite almost a decade of the AAP recommending that bronchodilators be used only if the infant shows a substantial clinical benefit from a trial dose.3 It is unclear why physicians continue to routinely use bronchodilators, but perhaps clinical judgment tells them it seems to help. The most recent AAP and CPS bronchiolitis guidelines, however, now strongly advise against even a trial of bronchodilators owing to lack of efficacy supported by, in addition to other sources, the 2014 Cochrane review discussed earlier. If adopted by front-line clinicians, this newest recommendation seems unlikely to have a positive impact on the current growing burden of viral wheezing in infants.
Complicating issues further, a largely ignored limitation in past studies of bronchiolitis is the inherent difficulty in delivering inhaled medications to the airways of small infants. In particular, we know that nebulized therapy will deliver about 5%–10% of the intended dose to the airways of cooperative older children,25 but this falls to less than 1% in crying infants struggling against a face mask.26 Thankfully, strategies now exist to dependably deliver about 2.5% of nebulized doses via a hood or head box.27 In infants, therefore, it is unclear whether our past inability to consistently show efficacy of inhaled asthma medications was due to a failure to respond or simply a failure to deliver.
Maybe there is no such thing as bronchiolitis
The time has come for a fundamental change in our approach to infants with viral wheezing. In most cases, we cannot know whether a wheezing infant has wheezed before or will again, and it seems unjustified to use “the first episode of wheezing” to arbitrarily distinguish bronchiolitis from preschool asthma. In fact, until we have the tools to confirm that these are indeed two separate diseases that can be distinguished by practical clinical or laboratory means, the use of labels such as bronchiolitis to avoid calling it asthma is unhelpful, may delay effective therapy and should be reconsidered. We must also re-evaluate past studies showing the lack of efficacy of asthma therapies in these infants, because they have been compromised by sampling errors, inherent difficulties in the delivery of inhaled medication and a lack of awareness of the therapeutic effect of inhaled saline. It seems more reasonable to accept that preschool asthma is a spectrum disorder that includes what we used to call bronchiolitis and that several age-related factors contribute to the observation that the condition is more difficult to treat in infants than in older children. Perhaps looking at wheezing infants from this perspective will lead us down a more productive path.
Key pointsRecently published guidelines for the diagnosis and management of viral bronchiolitis in infants seem to agree that bronchiolitis is a very common illness with no treatment options other than supportive care and, perhaps (based on “weak” evidence), inhaled hypertonic saline for inpatients only.
However, studies involving infants with viral lower respiratory tract obstruction have been limited to those experiencing their “first episode” of wheezing, which excludes many potentially eligible participants and weakens the evidence base.
Asthma in preschoolers is increasingly well understood, and there is perhaps a reasonable argument for considering that bronchiolitis may be merely an early episode of asthma, as there is overlap between triggers and causes.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
References
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

