


Abstract
Background: Operative vaginal delivery (OVD) is considered safe if carried out by trained personnel. However, opportunities for training in OVD have declined and, given these shifts in practice, the safety of OVD is unknown. We estimated incidence rates of trauma following OVD in Canada, and quantified variation in trauma rates by instrument, region, level of obstetric care and institutional OVD volume.
Methods: We conducted a cohort study of all singleton, term deliveries in Canada between April 2013 and March 2019, excluding Quebec. Our main outcome measures were maternal trauma (e.g., obstetric anal sphincter injury, high vaginal lacerations) and neonatal trauma (e.g., subgaleal hemorrhage, brachial plexus injury). We calculated adjusted and stabilized rates of trauma using mixed-effects logistic regression.
Results: Of 1 326 191 deliveries, 38 500 (2.9%) were attempted forceps deliveries and 110 987 (8.4%) were attempted vacuum deliveries. The maternal trauma rate following forceps delivery was 25.3% (95% confidence interval [CI] 24.8%–25.7%) and the neonatal trauma rate was 9.6 (95% CI 8.6–10.6) per 1000 live births. Maternal and neonatal trauma rates following vacuum delivery were 13.2% (95% CI 13.0%–13.4%) and 9.6 (95% CI 9.0–10.2) per 1000 live births, respectively. Maternal trauma rates remained higher with forceps than with vacuum after adjustment for confounders (adjusted rate ratio 1.70, 95% CI 1.65–1.75) and varied by region, but not by level of obstetric care.
Interpretation: In Canada, rates of trauma following OVD are higher than previously reported, irrespective of region, level of obstetric care and volume of OVD among hospitals. These results support a reassessment of OVD safety in Canada.
Operative vaginal delivery (OVD) refers to forceps- or vacuum-assisted delivery used in the second stage of labour to facilitate vaginal birth when labour is arrested, to expedite delivery when there is imminent risk to the fetus or to avoid exertion for people with conditions that contraindicate pushing.1 The choice of forceps or vacuum application is based on factors such as the presence of marked caput or moulding, access to epidural anesthesia, safety of expulsive efforts, gestational age, fetal presentation, and operator and patient preference.2,3
In the second stage of labour, OVDs are alternatives to cesarean delivery, which can be challenging and result in serious maternal and perinatal morbidity.3 Although no randomized controlled trials have compared outcomes following OVD and cesarean delivery,4,5 recent observational studies in high-income countries have found that cesarean delivery in the second stage of labour is associated with higher rates of maternal infection and neonatal respiratory morbidity compared with OVD.6–9 However, OVDs are associated with important maternal and neonatal complications, most notably, severe maternal and neonatal trauma.5–9 Maternity care providers and pregnant people in their care are thus tasked with weighing the trauma risks of OVD with the surgical risks of cesarean delivery, often when delivery is urgent.
In recent years, OVD has accounted for 10%–15% of deliveries in Canada,10 Australia11 and the United Kingdom,12 where guidelines affirm the safety of OVD when performed appropriately by trained personnel.12–14 However, the risk associated with OVD is heavily dependent on the health provider’s expertise, and the declining use of OVD (in favour of cesarean delivery) has reduced opportunities for acquiring proficiency in performing these deliveries, especially with forceps.10,15,16 As a result, OVD is under scrutiny in the face of reports of rising rates of maternal and neonatal trauma with OVD and of concerns regarding the relative safety of forceps versus vacuum.17–19
An evaluation of maternal and neonatal trauma following OVD is necessary to ensure that health care providers, policy-makers and pregnant people are informed regarding the risks of OVD typically experienced in routine obstetric practice, as opposed to those encountered in ideal conditions. Further, although enhanced training in OVD has been deemed urgent,3,12,16 little information is available to guide decisions on which centres in Canada are best suited to lead such training initiatives. 20,21 Thus, we aimed to describe the incidence of maternal and neonatal trauma following OVD in Canada and to quantify the variability in trauma rates by instrument, region, level of obstetric care and institutional OVD volume.
Methods
Study design and population
We conducted a cohort study of deliveries in Canada between April 2013 and March 2019, excluding Quebec. We included all singleton, term (≥ 37 weeks), in-hospital deliveries to pregnant people without a previous cesarean delivery that resulted in a live birth or stillbirth.
Data sources
We obtained data about hospital deliveries from the Canadian Institute for Health Information’s (CIHI) Discharge Abstract Database, which contains information on 98% of hospital deliveries in Canada, excluding those in Quebec.22 Trained health records personnel abstract information from the databases using standardized definitions, and data consistency and accuracy are ensured through routine quality assurance checks.
Maternal, fetal and neonatal information in the database includes details regarding medical history, maternal characteristics, labour and delivery, neonatal condition, diagnoses and interventions. Diagnoses are coded using the International Classification of Diseases, 10th revision23 (ICD-10-CA), and interventions are coded using the Canadian Classification of Health Interventions (Appendix 1, Table S1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.210841/tab-related-content).24 The accuracy of the perinatal information in the databases has been validated in previous studies (Appendix 1, Table S2).25–27
Outcomes
The primary outcomes were composite maternal trauma and composite neonatal trauma. We quantified maternal trauma rates among all deliveries, and quantified neonatal trauma rates for live births without a congenital malformation. Maternal trauma included obstetric anal sphincter injury (OASI), defined as third- or fourth-degree perineal tears; cervical or high vaginal laceration; pelvic hematoma; obstetric injury to the pelvic organs, pelvic joints or ligaments; injury to the bladder or urethra; and other pelvic trauma. Neonatal trauma included intracranial hemorrhage and laceration, skull fracture, severe injury to the central nervous system (e.g., cerebral edema, brain damage, injury to the cranial nerves, spine or spinal cord) or to the peripheral nervous system (e.g., Erb paralysis, brachial plexus injury, Klumpke paralysis), fracture of the long bones, injury to the liver or spleen, seizures, neonatal death) (Appendix 1, Table S1).
Statistical analysis
We stratified deliveries by mode of delivery using an intention-to-treat framework. For example, we included cesarean delivery after a failed forceps attempt in the attempted forceps delivery group. We calculated crude rates of maternal and neonatal trauma among spontaneous vaginal deliveries and OVDs to provide context. We did not make any direct comparisons between trauma rates following OVD and spontaneous vaginal deliveries since confounding by indication compromises such contrasts. However, we estimated adjusted incidence rate ratios (IRRs), adjusted number needed to treat and 95% confidence intervals (CIs) using log-binomial regression for outcomes among forceps versus vacuum deliveries. Adjusted models included maternal province or territory of residence, age, parity, hypertension, diabetes, fetal distress during labour, pelvic station (i.e., outlet, low, midpelvic),13 post-term gestation (≥ 42 weeks), and fetal macrosomia (≥ 4000 g). We included missing values for parity (7.0%) and for pelvic station (7.7% for forceps, 34.8% for vacuum) in the multivariable models using a “missing” category.
We further compared rates of trauma related to OVD by region (i.e., province or territory) and by level of obstetric care. We stabilized trauma rates to account for the imprecision introduced by units with small numbers by grouping data from the 3 territories into a “combined territories” category and by using mixed-effects logistic regression.28 The regression models included the same covariates listed above as fixed effects (to adjust risk for case mix) and a random intercept term, specific to the unit of comparison (i.e., province or territory, level of obstetric care). Additionally, we estimated the relationship between the OVD rate and trauma rates for each province or territory by year using the coefficient of determination (R2).
We evaluated outcome rates across tiers of service by province. Level of obstetric care in Canadian hospitals is designated by tier, ranging from tier 0 to tier 3 or 4, which reflects the availability of increasing complexity of care. Tier of service classifications are province- and territory-specific.29,30 We excluded hospitals in tiers 0 and 1 since OVD is uncommon or not supported in such institutions. For simplicity, we conducted this analysis for only British Columbia, Alberta and Ontario.
Lastly, we quantified the association between volume of OVD at the hospital level and rates of trauma, while adjusting for the same covariates, using ecologic Poisson regression.31 Each hospital-year represented 1 unit of analysis (e.g., hospital A in 2013, hospital B in 2014). We evaluated the possibility of a nonlinear relationship between hospital OVD volume and the frequency of maternal trauma following OVD using a nonparametric model, smoothed using restricted cubic splines with 5 knots.32 We tested for nonlinearity using the likelihood ratio test and compared the linear and smoothed models.
Ethics approval
We obtained ethics approval for the study from the University of British Columbia (H17–00587).
Results
We included 1 326 191 singleton deliveries at ≥ 37 weeks’ gestation in pregnant people without a previous cesarean delivery. Of these, 38 500 (2.9%) were attempted forceps deliveries and 110 987 (8.4%) were attempted vacuum deliveries (Figure 1). These deliveries resulted in 1 236 037 live births without congenital malformations (Appendix 2, Figure S1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.210841/tab-related-content). Forceps and vacuum deliveries were more frequent among nulliparous than parous people, and in deliveries with fetal distress. Vacuum was more commonly used than forceps at all pelvic stations (Table 1). Of the 38 500 attempted forceps deliveries, 1606 (4.2%) failed, and 8791 (7.9%) of the 110 987 attempted vacuum deliveries failed (Appendix 1, Table S3).
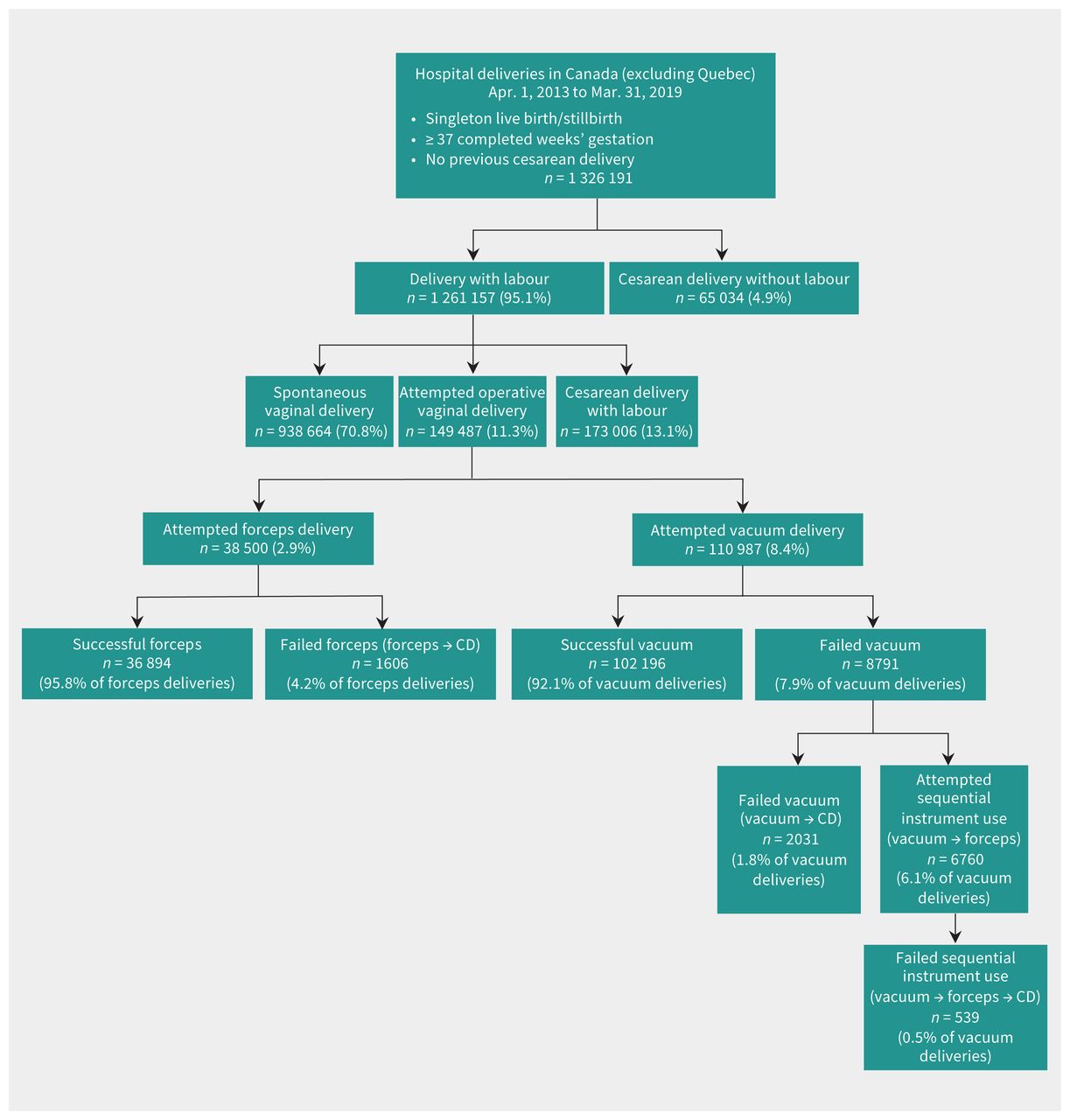
Distribution of deliveries included in the study by mode of delivery. Note: CD = cesarean delivery.
Maternal, delivery and neonatal characteristics by mode of delivery in pregnant people without a previous cesarean delivery
Maternal trauma
Maternal trauma occurred in more than one-quarter of deliveries with forceps (n = 9728, 25.27%, 95% CI 24.83% to 25.70%) (Table 2) and 14 614 (13.17%, 95% CI 12.97% to 13.37%) vacuum deliveries (adjusted IRR 1.70, 95% CI 1.65 to 1.75). The frequency of OASI was particularly high with forceps delivery (21.52% v. 11.67% with vacuum) and accounted for most of the maternal trauma with forceps and vacuum. The rate of fourth-degree perineal laceration was 2.20% with forceps and 1.22% with vacuum.
Maternal trauma and neonatal trauma among pregnant people with a spontaneous vaginal delivery, attempted forceps delivery or attempted vacuum delivery
Neonatal trauma
The rate of neonatal trauma was similar for forceps (9.56 per 1000 live births, 95% CI 8.58 to 10.62) and vacuum delivery (9.58 per 1000 live births, 95% CI 8.99 to 10.18) (Table 2). Severe injury to the peripheral nervous system, the most frequent neonatal trauma, was more common following forceps (4.85 per 1000 live births, 95% CI 5.16 to 5.63) than vacuum (3.41 per 1000 live births, 95% CI 3.06 to 3.78) (adjusted IRR 1.33, 95% CI 1.08 to 1.65). Conversely, the rate of subgaleal hemorrhage was higher with vacuum (forceps v. vacuum adjusted IRR 0.28, 95% CI 0.19 to 0.42). Absolute rates of neonatal trauma were low (Table 2).
Trauma rates by region
The crude rate of forceps delivery varied widely by region (from 0.4% to 4.1%), a finding that remained after adjustment and stabilization (Appendix 1, Table S4). The adjusted rate of maternal trauma with forceps delivery also varied widely, from 17.7% to 41.0% (Figure 2A; Appendix 1, Table S4). Adjusted rates of neonatal trauma following forceps delivery ranged from 0.0 to 10.3 per 1000 live births; regions with nonzero rates did not vary significantly (Figure 2B). There was less regional variation in adjusted rates of vacuum delivery (6.7% to 9.9%; Appendix 1, Table S5), although adjusted rates of maternal trauma following vacuum delivery ranged from 8.4% to 20.0% (Figure 2A). Adjusted rates of neonatal trauma following vacuum delivery were similar across provinces (Figure 2B; Appendix 1, Table S5).

Rates of (A) maternal and (B) neonatal trauma following attempted forceps delivery, attempted vacuum delivery and spontaneous vaginal delivery, for all of Canada (CA), excluding Quebec, and stratified by province or territory (April 2013 to March 2019). We adjusted and stabilized rates using mixed-effects logistic regression. Note: CI = confidence interval, CT = Combined territories.
We observed a positive linear relationship between the OVD rate and the maternal trauma rate in a province or territory in a given year (R2 = 0.42, p < 0.0001) but no association between OVD rate and neonatal trauma rate (R2 = 0.01, p = 0.5; Appendix 2, Figure S2).
Trauma rates by level of care
In British Columbia, Alberta and Ontario, the rates of maternal trauma were significantly higher with forceps than vacuum deliveries, and were similar across levels of obstetric care (Figure 3). Neonatal trauma rates were similar following forceps and vacuum delivery and did not vary with level of care (Appendix 2, Figure S3).

Maternal trauma rates following attempted forceps and attempted vacuum delivery by tier of obstetric service in (A) British Columbia, (B) Alberta and (C) Ontario (April 2013 to March 2019). We adjusted and stabilized rates using mixed-effects logistic regression. Analysis by tier of service was province- or territory-specific, as these frameworks varied across jurisdictions. Numeric (e.g., Tier 1, Tier 2, Tier 3) or alphanumeric (Tier 1, Tier 2A, Tier 2B) labels are used to identify tiers of obstetric service with increasing complexity of care.29 Note: CI = confidence interval.
Trauma rates by hospital OVD volume
We included 1853 hospital-years in the ecologic Poisson regression. The adjusted rate of maternal trauma with forceps delivery decreased when hospital forceps use increased to 30 forceps deliveries per year (Figure 4A). We did not observe a relation between volume of forceps delivery and maternal trauma above this threshold, however, and most hospitals had average trauma rates of 23%–25%. For vacuum deliveries, we observed a complex nonlinear relation in maternal trauma rates, with increasing vacuum use at low volume, but there was no relation between volume and trauma rate among hospitals performing more than about 200 vacuum deliveries per year, where the maternal trauma rate was 14%–16% (Figure 4B). The adjusted rate of neonatal trauma was not associated with hospital volume of OVD (Appendix 2, Figure S4).
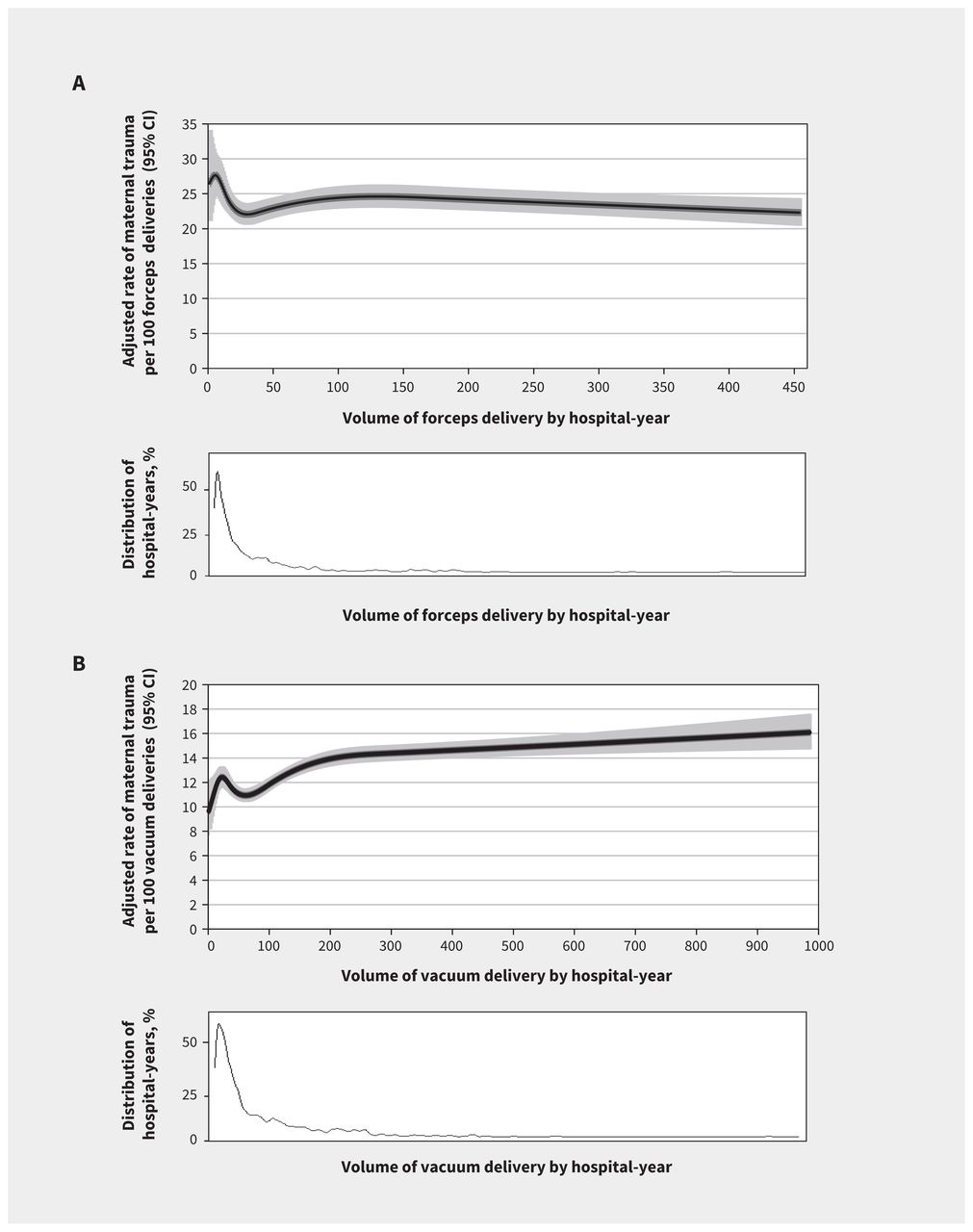
Rates of maternal trauma per 100 (A) forceps deliveries and (B) vacuum deliveries by the annual volume of forceps delivery in each hospital, and distribution of hospital-years by annual forceps volume (April 2013 to March 2019). We adjusted and stabilized rates using mixed-effects logistic regression. Note: CI = confidence interval.
Discussion
We evaluated the frequency of maternal and neonatal trauma following attempted forceps and attempted vacuum delivery in Canada (excluding Quebec), and stratified our analyses by region, level of obstetric care and hospital OVD volume. Maternal trauma rates were highest with forceps delivery, with more than 1 in 4 deliveries affected by maternal trauma and 1 in 105 infants affected by neonatal trauma. Maternal and neonatal trauma following vacuum deliveries occurred in 1 in 8 deliveries and 1 in 104 infants, respectively. Rates of OVD and maternal trauma following OVD varied substantially by region, with a positive correlation between the frequency of OVD use and maternal trauma. We did not observe any differences in trauma rates following OVD by level of obstetric care, nor was there a clear association between trauma and hospital volumes of OVD.
Despite rates of OVD similar to those in Canada, the rate of OASI following OVD is substantially lower in the UK (8%–12% with forceps and 1%–4% with vacuum)12 and in Australia (9.3%–14.1% with forceps and 5.4%–5.9% with vacuum; Table 3).14 The Organisation for Economic Co-operation and Development (OECD) reported that the 2015 rate of maternal trauma following OVD in Canada greatly exceeded that of any other OECD country (Appendix 2, Figure S5).33 Some of this variability is likely from differences in documentation and reporting, but clinician selection of patients, skill and choice of instrument are other potential causes.34 Variation in policy regarding the use of episiotomy in OVD may also be a factor. Accumulating evidence supports the routine use of mediolateral episiotomy in OVD, particularly among people having their first vaginal delivery,35–38 yet recommendations surrounding episiotomy in OVD are inconsistent across countries. The Royal Australian and New Zealand College of Obstetricians and Gynaecologists recommends use of routine episiotomy for all people having their first vaginal birth and requiring OVD,14 but restrictive use of mediolateral episiotomy in OVD is recommended in Canada. 13 In a 2020 report from the UK, episiotomy was used in 90% of deliveries with forceps and 50%–60% of vacuum deliveries. 12 Equivalent rates in Canada were 65% and 38%, respectively, in 2018.35
In our study, OASI occured in 87% of deliveries with maternal trauma following OVD and accumulating evidence shows the severe long-term consequences of these injuries,39–44 such as urinary and fecal incontinence, dyspareunia and other pelvic floor disorders.39,40 Reported rates of anal incontinence following the primary repair of OASI are between 15% and 61% (mean 39%),41,42 and these increase with time, from 31% at 3–6 months to 54% at 3–8 years following delivery.43 The frequency of OASI found in our study (21.5% with forceps and 11.7% with vacuum), compared with those reported in current OVD guidelines (4.0%– 6.6% of all vaginal births) (Table 3), highlights the importance of reporting timely, empirically derived measures of risk that reflect the risks pregnant people actually encounter in typical obstetric practice.
Morbidity following OVD needs to be compared with potential alternatives to OVD. These include an extended second stage of labour and a spontaneous vaginal delivery, or a second-stage cesarean delivery, both of which are associated with serious morbidity.5–7,45 However, the high population rates of morbidity following OVD also raise questions about the choice of instrument, obstetrician training in OVD use and the potential ability to recognize patients who would benefit from a cesarean delivery earlier in labour. In our study, rates of maternal trauma following OVD were high among all levels of obstetric care. Further study of optimal training environments is warranted.
Limitations
Some degree of misclassification in diagnoses and interventions recorded in large databases is inevitable. However, several studies have validated the information in the Discharge Abstract Database used in this study (Appendix 1, Table S2),25–27 and the data are abstracted by trained medical records personnel using standardized rules, with oversight by CIHI. A related report46 on the safety of OVD in the 386 hospitals included in this study showed large variations among hospitals in the type of instrument used and trauma rates, suggesting major differences among hospitals in obstetric practice (including indication for use and skill of obstetrician). Although measurement of pelvic station can be subjective and affected by moulding and fetal head position,47 our data reflect the current norms of diagnosis by contemporary maternity care providers in Canada. We lacked information on the pregnant person’s predisposition to trauma (e.g., family history of pelvic floor dysfunction), body mass index, multiple deliveries, rotational or nonrotational OVD, and the class of third-degree perineal laceration, which limits a more nuanced understanding of variations in trauma rates.
Conclusion
Rates of maternal and neonatal trauma following OVD are high in Canada compared with other countries with similar rates of OVD, and are especially high in some provinces. These high rates call for a reassessment of the safety of OVD, not just in Canada, but in all settings where the rates of OVD and the opportunities for training in OVD are changing. Although OVDs may be associated with low rates of morbidity in carefully selected circumstances, the high rates of trauma following forceps and vacuum deliveries, documented across regions, levels of obstetric care and hospitals, show that such ideal conditions do not apply to obstetric practice in Canada.
Acknowledgement
The authors would like to acknowledge the contribution of the members of the Canadian Institutes of Health Research Team on Regionalized Perinatal Health Care. A list of team members and affiliations can be found at https://phsr.obgyn.ubc.ca/members/
Footnotes
Competing interests: Michael Kramer reports funding from the Canadian Institutes of Health Research and the Family Rosenquist Foundation, outside the submitted work. He also reports participation on the data safety monitoring board of the MOBYDick clinical trial and on the scientific advisory board of the Family Rosenquist Foundation.
This article has been peer reviewed.
Contributors: Giulia Muraca and KS Joseph proposed the study concept and design, and conducted the analyses. Amélie Boutin, Neda Razaz, Sarka Lisonkova, Sid John, Joseph Ting, Heather Scott and Michael Kramer interpreted the data. Giulia Muraca drafted the manuscript. All the authors reviewed the manuscript critically for intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Giulia Muraca is supported by a Canadian Institutes of Health Research (CIHR) Postdoctoral Fellowship. Amélie Boutin is supported by a Killam Postdoctoral Research Fellowship Award and a Fellowship Award from CIHR. Neda Razaz is supported by the Swedish Research Council for Health, Working Life and Welfare (DNR 4-2707/2019). Sarah Lisonkova is supported by a Scholar Award from the Michael Smith Foundation for Health Research. KS Joseph is supported by an Investigator award from the BC Children’s Hospital Research Institute. This study was funded by a Canadian Institutes of Health Research Team grant (PER-150902) on perinatal care regionalization in Canada.
Data sharing: These data were acquired from the Canadian Institute for Health Information (CIHI). Access to these data is available to researchers, health managers and decision-makers via a formal data request process administered by CIHI. More information on the data holdings and the request process is available at: www.cihi.ca/en/access-data-and-reports/make-a-data-request.
- Accepted September 27, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

Article tools






{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Airway obstruction resulting from massive subgaleal hematoma caused by superficial temporal artery injuries in an adult patient with liver cirrhosis
- Relationship Between Neonatal Brain Injury and Objective Measures of Head Trauma: A Case-Control Study
- Maternal and neonatal trauma during forceps and vacuum delivery must not be overlooked
- Long-term neurodevelopmental outcome in children born after vacuum-assisted delivery compared with second-stage caesarean delivery and spontaneous vaginal delivery: a cohort study
- The authors reply regarding transparency, balance and perspective on intervention at full dilation
- A balanced perspective on intervention at full dilation
- Intrapartum ultrasonography may improve operative vaginal delivery outcomes in Canada
More in this TOC Section
Similar Articles
Collections


Podcast