


Abstract
Background: During the first year of the COVID-19 pandemic, the proportion of reported cases of COVID-19 among Canadians was under 6%. Although high vaccine coverage was achieved in Canada by fall 2021, the Omicron variant caused unprecedented numbers of infections, overwhelming testing capacity and making it difficult to quantify the trajectory of population immunity.
Methods: Using a time-series approach and data from more than 900 000 samples collected by 7 research studies collaborating with the COVID-19 Immunity Task Force (CITF), we estimated trends in SARS-CoV-2 seroprevalence owing to infection and vaccination for the Canadian population over 3 intervals: prevaccination (March to November 2020), vaccine roll-out (December 2020 to November 2021), and the arrival of the Omicron variant (December 2021 to March 2023). We also estimated seroprevalence by geographical region and age.
Results: By November 2021, 9.0% (95% credible interval [CrI] 7.3%–11%) of people in Canada had humoral immunity to SARS-CoV-2 from an infection. Seroprevalence increased rapidly after the arrival of the Omicron variant — by Mar. 15, 2023, 76% (95% CrI 74%–79%) of the population had detectable antibodies from infections. The rapid rise in infection-induced antibodies occurred across Canada and was most pronounced in younger age groups and in the Western provinces: Manitoba, Saskatchewan, Alberta and British Columbia.
Interpretation: Data up to March 2023 indicate that most people in Canada had acquired antibodies against SARS-CoV-2 through natural infection and vaccination. However, given variations in population seropositivity by age and geography, the potential for waning antibody levels, and new variants that may escape immunity, public health policy and clinical decisions should be tailored to local patterns of population immunity.
The COVID-19 pandemic defied expectations about immunity arising from infection and vaccination. During the first months of the pandemic, despite the burden on Canadian society and health systems, rates of symptomatic infection remained low, with 580 000 confirmed cases by December 2020, representing 1.6% of the Canadian population.1 Vaccines were widely distributed in Canada beginning in early 2021, with a rapid rise in vaccine coverage to 79% by fall of 2021,2 whereas cumulative reported cases of COVID-19 remained low, at 4.7% of the population.3 The arrival of Omicron variants and subvariants, however, caused an unprecedented increase in the number of infections. In short, the high vaccine coverage, combined with population immunity from infections in earlier waves of the pandemic, were insufficient to slow the spread of the Omicron variant.
Although the overall progression of confirmed cases and vaccination is clear, the underlying dynamics of population seropositivity are less obvious, yet critically important for policy and clinical decisions about vaccination and other preventive measures. A count of confirmed cases of COVID-19 is of limited use for understanding the evolution of population immunity because case ascertainment is biased by multiple factors. Most notably, access to laboratory-based polymerase chain reaction (PCR) testing varied across the country and, in many locations, was overwhelmed by demand after December 2021. In this context, serological surveillance provides an informative adjunct to monitoring confirmed cases, as seroprevalence offers a more direct measure of population humoral immunity.
We sought to describe the trajectory of SARS-CoV-2 seroprevalence in the Canadian population, as measured by anti-nucleocapsid (anti-N) and anti-spike protein (anti-S) antibody levels over 3 intervals: prevaccination (March to November 2020), vaccine roll-out (December 2020 to November 2021), and the Omicron variant waves (December 2021 to March 2023). We draw on seroprevalence estimates from multiple studies collaborating with the COVID-19 Immunity Task Force (CITF).4 In addition to describing the temporal evolution of population seropositivity in Canada, we highlight trends in infection-acquired and vaccine-induced seroprevalence by Canadian region and age.
Methods
Data sources
We used aggregate data reported by research studies collaborating with the CITF, which began supporting studies measuring SARS-CoV-2 seroprevalence across Canada in April 2020. For this analysis, we used seroprevalence estimates reported by 7 studies (Table 1), covering 3 time intervals: prevaccination, March 2020 to November 2020; vaccine roll-out, December 2020 to November 2021; and the Omicron variant waves, December 2021 to March 2023 (see Appendix 1, Supplemental Table 1S, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.230249/tab-related-content, for study summaries by time period). Most individual observations and seroprevalence estimates were from blood donors, who are adults older than 17 years, but some estimates were from provincial laboratory studies, which tested residual blood samples from people of all ages. There was a slight predominance of males among blood donors, but most provincial residual blood samples and other studies were more evenly matched for sex. Residual blood samples from Saskatchewan and the Canadian Partnership for Tomorrow’s Health, a pan-Canadian cohort consortium that recruited participants from the general population, were predominantly from females. The sampling frequency ranged from biannually to monthly, and the total number of people sampled at each time point across all provinces (if applicable) ranged from 12 to 77 000 (median 6700). In total, more than 900 000 individual samples from 10 provinces contributed to the seroprevalence estimates included in the analysis.
Sources of data on Canadian population seroprevalence and sample descriptors
Measurement of SARS-CoV-2 immunity, serological assays and seroprevalence estimates
Humoral immunity to SARS-CoV-2 was measured in blood samples obtained through venous blood draws or finger-prick samples placed on filter paper (dried blood spots). Assays detected immunoglobulin G (IgG) antibodies against SARS-CoV-2 nucleocapsid (anti-N), spike (anti-S) proteins, or receptor binding domain (anti-RBD) proteins. Because RBD is a component of the S-protein complex, anti-S and anti-RBD were grouped together to measure anti-S seroprevalence. Before vaccination was widely available in January 2021, detection of either anti-N or anti-S was taken as evidence of infection-acquired seropositivity. After December 2020, only anti-N was taken as evidence of infection-acquired seropositivity, and anti-S was taken as evidence of vaccine-induced or infection-acquired seropositivity.
Some studies used commercially available assays (e.g., Abbott Laboratories, Roche, DiaSorin) and other studies used assays developed in academic laboratories (e.g., Mount Sinai Hospital, University of Ottawa, Université de Montréal) (Appendix 1, Supplemental Table 2S and Supplemental Table 3S). Commercial assays were performed according to the manufacturer’s specifications, and assays developed in academic laboratories were performed according to their standardized protocols.5 Given the variety of assay measurements used, we estimated seroprevalence within each study as the proportion of people who tested positive for anti-N or anti-S antibodies using thresholds for positivity defined by the manufacturer or published protocol. Most seroprevalence estimates were age and sex standardized to the general population (Table 1). We adjusted estimates by sensitivity and specificity using the Rogan–Gladen estimator6 to account for the accuracy of the assay.
Statistical analysis
Our main objective was to estimate seroprevalence for the general population in Canada overall, and the provinces (excluding the territories) during 3 intervals: prevaccination (March–November 2020), vaccination roll-out (December 2020–November 2021), and the Omicron variant waves (December 2021–March 2023). As a secondary objective, we described trends in seroprevalence by age groups (< 25 yr; 25–39 yr; 40–59 yr; ≥ 60 yr) and geographical regions.
We used a time-series approach to estimate trends in SARS-CoV-2 infection–induced seroprevalence (anti-N and anti-S prevaccination; anti-N postvaccination) and seroprevalence owing to infection or vaccination (anti-S) for the Canadian population. We conducted the analysis using a Bayesian framework and generalized linear multilevel models for β-binomial distributed outcomes (for model specification and a description of how we tested for differences among provinces and age groups, see Appendix 2, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.230249/tab-related-content). We conducted the analysis using R version 4.3 (Apr. 21, 2023) and JAGS 4.3.1.
Ethics approval
All studies contributing data to this article obtained ethical approval from local institutional review boards for use of the samples. Data were provided to the CITF in aggregate form, such that it was not possible to re-identify individuals. The analysis of the data contributed by studies was approved by the McGill Faculty of Medicine and Health Sciences Institutional Review Board.
Results
After the initial epidemic wave and before the availability of vaccines, less than 0.3% (95% credible interval [CrI] 0.02%–0.9%) of the Canadian population had either anti-S or anti-N antibodies in July 2020, and the average monthly increase in anti-N seroprevalence was 0.05% (95% CrI 0.01%–0.11%) in 2020 (Figure 1). Seroprevalence owing to infection continued to increase slowly during vaccine roll-out, at an average of 0.39% (95% CrI 0.25%–0.53%) per month from January 2021 to Dec. 15, 2021, reaching 9.0% (95% CrI 7.3%–11%) in November 2021. Despite high vaccine coverage in Canada, all previous increases in seroprevalence were far surpassed by the increase caused by the Omicron variant. After 6 months of the Omicron variant circulating in Canada, seroprevalence had risen to 47% (95% CrI 45%–49%) by mid-June 2022, with an average monthly increase of 6.4% per month (95% CrI 6.1%–6.8%) between Dec. 15, 2021, and July 2022. After a short interval of slower increases in the summer, infection-acquired seroprevalence continued to rise rapidly in the latter half of 2022 until it started to plateau at about 76% (95% CrI 74%–79%) in March 2023. The rate of increase in the Omicron era varied from a peak of 9% per month (95% CrI 7.1%–10%) in February 2022 to lows of around 1% to 2% per month since December 2022.

SARS-CoV-2 infection–acquired and vaccine–induced seroprevalence in Canada (March 2020 to March 2023). Anti-nucleocapsid (anti-N) and anti-spike (anti-S) seropositivity for all age groups combined, by region. Each point represents a seroprevalence estimate from a project at the midpoint of a sample collection period, including all age groups. Infection-acquired seropositivity was measured as anti-N or anti-S seropositivity before January 2021, but only anti-N seropositivity after December 2020. The solid and dashed black lines represent the population-weighted mean of the anti-N and anti-S seroprevalence Bayesian model estimates, respectively. The grey bands represent the 95% credible intervals. Atlantic provinces: New Brunswick, Nova Scotia, Newfoundland and Labrador, Prince Edward Island; Eastern Canada: Ontario, Quebec; Western Canada: Manitoba, Saskatchewan, British Columbia, Alberta, the Northwest Territories.
Estimates of seropositivity for anti-S IgG antibodies, reflecting previous vaccination or infection, were between 70% and 95% in summer 2021, depending on the source of the samples, with a mean of 85% (95% CrI 81%–89%; Figure 1) around Aug. 1, 2021. The prevalence of anti-S antibodies was largely attributable to vaccination as it increased rapidly after March 2021 despite the small increases in anti-N antibodies. On average, anti-S seroprevalence was consistently high — 98% or higher — from November 2021 through the Omicron variant waves.
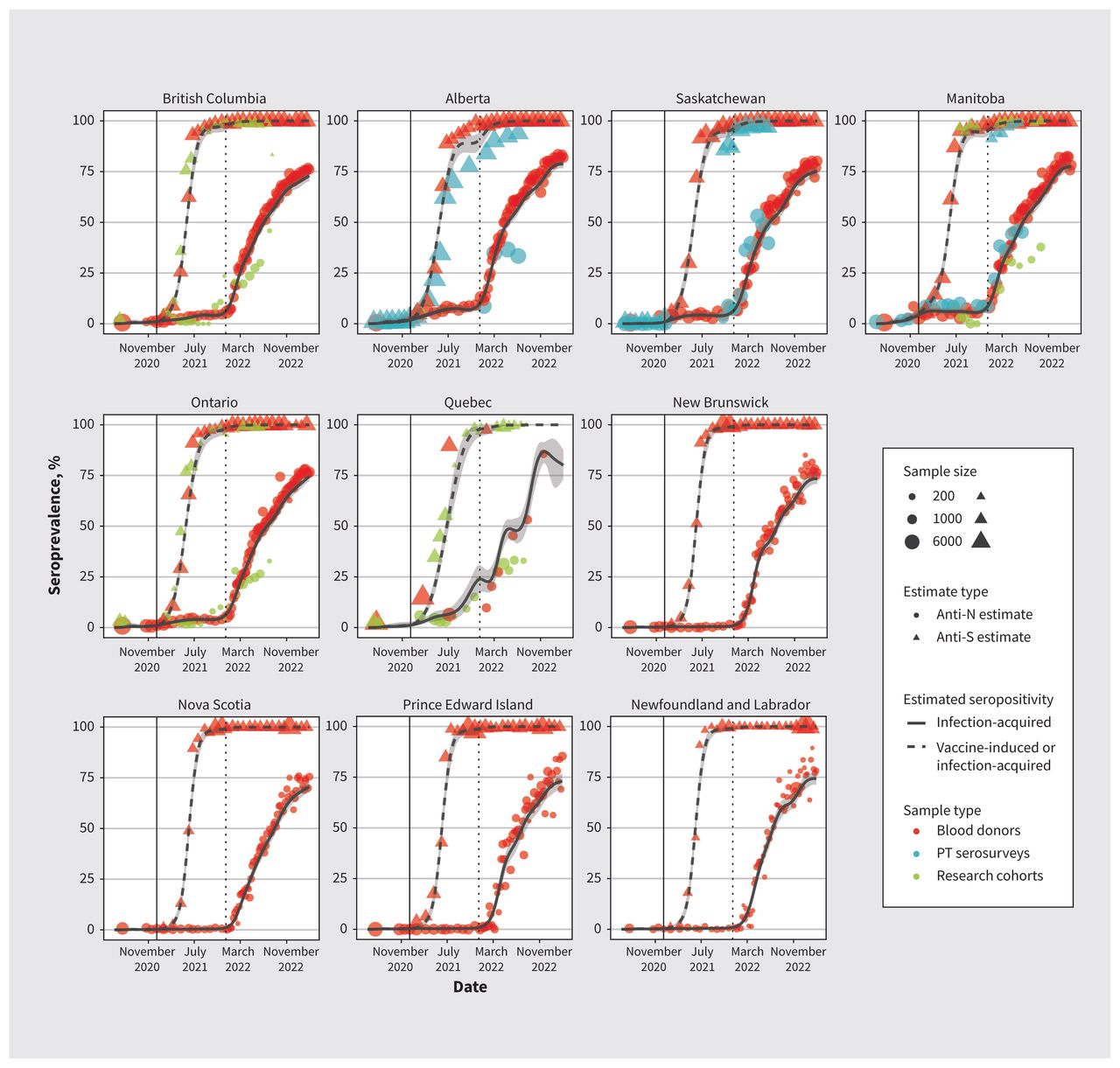
Anti-N seroprevalence followed a similar trajectory in most provinces throughout the pandemic (Figure 2). The Atlantic provinces were a notable exception, with infection-acquired seroprevalence consistently below 1% pre-Omicron variant waves, possibly a result of the policies restricting travel into and out of the Atlantic provinces. Nevertheless, infection-acquired seropositivity rose subtantially in the Atlantic provinces during the Omicron variant waves and was comparable to that in other provinces 1 year later. In November 2022, seroprevalence ranged from 64% (95% CrI 61%–67%) in Nova Scotia to 74% (95% CrI 70%–75%) in Alberta. Compared with Ontario, the relative risk for Nova Scotia was 0.96 (95% CrI 0.90–1.01) in November 2022, but it had been 0.14 (95% CrI 0.08–0.23) in November 2021; the relative risk for Alberta was 1.10 (95% CrI 1.03–1.20) in November 2002, but it had been 1.67 (95% CrI 1.20–2.29) in November 2021. The estimates were not sensitive to the choice of previous distributions for the between-province variability in model parameters, except for Quebec, where the available data were sparse (Appendix 2, Supplementary materials Section 3).

SARS-CoV-2 infection–acquired and vaccine–induced seroprevalence (March 2020 to March 2023). Anti-nucleocapsid (anti-N) and anti-spike (anti-S) seropositivity estimates by province and sample type. Each point represents a seroprevalence estimate from a project at the midpoint of a sample collection period. The solid and dashed black lines represent the average anti-N and anti-S seroprevalence, respectively, estimated from a Bayesian hierarchical model that accounts for sample size. The grey bands represent the 95% credible intervals. See the Methods section for details of the statistical model. Note: PT = provincial and territorial.
Before the Omicron waves, infection-acquired seroprevalence differed little by age (Figure 3), but during the Omicron waves, rates of seropositivity increased more quickly in younger age groups. By mid-June 2022, infection-acquired seroprevalence in people younger than 25 years was highest (57%), followed by those aged 25–39 years (51%), those aged 40–59 years (40%), and those aged 60 years and older (25%). We also observed this trend in data from provincial serosurveys, in which children and adolescents had the highest seroprevalence. Except in adults older than 65 years, seroprevalence was between 70% and 80% by March 2023, age differences having decreased. Compared with adults aged 50–59 years, the relative risk for those aged 18–29 years was 1.13 (95% CrI 1.11–1.16) in March 2023, but it had been 1.52 (95% CrI 1.47–1.57) in June 2022.

SARS-CoV-2 infection–acquired seroprevalence. Anti-nucleocapsid (anti-N) seropositivity estimates by age group (March 2020 to March 2023). Each age-stratified seroprevalence estimate reported is plotted both at the centre of the age stratum and the midpoint of the temporal sampling interval. Each estimate is plotted at the midpoint of the sample collection period and coloured for the corresponding age group. The coloured trend lines represent the average anti-N seroprevalence estimated from a Bayesian hierarchical model that accounts for sample size. The coloured bands represent the 95% credible intervals. See the Methods section for details of the statistical model.
Interpretation
During the prevaccine and vaccine roll-out intervals, relatively few people in Canada had evidence of humoral immunity to SARS-CoV-2 from an earlier infection. This changed rapidly during the Omicron era; by September 2022, most of the population had detectable antibodies from infection. The rise in infection-induced humoral immunity occurred rapidly across all geographical regions and age groups in Canada. This rapid rise in seropositivity owing to infection occurred despite the roll-out of vaccines in 2021, which led to high rates of vaccine-induced antibodies detected across the country,7 protecting most people in Canada from severe illness and death.7 However, this high vaccine coverage did not prevent the unprecedented transmission and epidemic growth of the Omicron variant in late 2021 and early 2022.8,9 Given the immune evasion and high transmissibility of the Omicron variant,10 most people in Canada now have infection-acquired immunity and vaccine-induced immunity, ushering in an era of hybrid immunity.11,12
The low infection rate in Canada before the arrival of the Omicron variant was observed in other high-income countries in North America and Europe.13 A rapid rise in anti-N seroprevalence during the Omicron era was also observed in these countries. In Finland, for example, similar age-specific trends were observed in a study of residual blood samples, where peak seroprevalence rose from less than 10% to about 30% in February 2022.14 In a study of residual blood samples in the United States, similar age-specific trends were seen, including a slower rise in anti-N among older adults during the Omicron era, with infection-induced seroprevalence over 60% for the 18- to 49-year age group by February 2022.15
The rapid rise in infection seen in many countries with high vaccine coverage is explainable, in part, by the limited effectiveness of the ancestral SARS-CoV-2 strain–based vaccines in preventing infection with the Omicron variant.16 This immune evasion, combined with the high transmissibility of the Omicron variant, allowed the epidemic to spread rapidly.
Although the Omicron wave caused similar increases in infection-induced humoral immunity in multiple countries, the implications for population immunity may vary, owing to differences in the sequence and timing of vaccination and infection in each jurisdiction. In Canada, before the Omicron era, most people had been vaccinated, but not infected. During the Omicron wave, most of the population were then infected, likely producing hybrid immunity that potentially could protect against infection for months.17,18 However, antibody levels also differ within Canada across geographical regions and age groups, likely a result of factors that we did not measure (e.g., occupation, booster vaccination status, comorbid conditions). Periodic serosurveillance in the general population in Canada, as well as vulnerable populations, will be important to track waning of serological markers.
By building on the collaboration of many researchers with the CITF, we were able to use the most comprehensive collection of SARS-CoV-2 seroprevalence estimates assembled for Canada. We also harnessed the ability of serology to distinguish between antibodies induced through infection and vaccination to clearly characterize the independent effects of vaccination and infection on population seroprevalence. Our results are consistent with those from a study in British Columbia19 but they further characterize interprovincial variations in Canada. This study is not only a comprehensive assessment of infection-induced immunity to SARS-CoV-2 in Canada, but also shows that serosurveys detect a much higher infection rate than studies using PCR-confirmed infections.
We believe that the lessons learned from our results include a need for Canada to approach pandemic-related problems in a multidisciplinary manner, aligning expertise in public health and pandemic responses with input from the broader scientific community. Although there is a need in a pandemic to rapidly develop vaccines that target a pathogen broadly, control spread and mitigate impacts, it is difficult to fully control pathogens that mutate rapidly through vaccination alone (although vaccination markedly decreased the severity of illness from those infected with SARS-CoV-2). Measurement and analysis of antibodies to vaccination and infection provide crucial information for clinicians and policy-makers, particularly when rapid emergence of mutations drastically changes interpretation of other sources of surveillance data, such as confirmed infections, hospital admissions and deaths. Although currently challenging to conduct at scale, assays that can give a broader overall picture of immunity, such as measures of cell-mediated immunity and neutralizing antibodies, could further extend our ability to monitor and understand the effects of vaccination and infection.
Limitations
Although these data were not sampled from a single cohort, many of the samples included were systematically repeated in the same populations. For most of the estimates used in this study, the population sampled was blood donors. This population does not include children or people from remote areas, but SARS-CoV-2 seroprevalence estimates from blood donors have been shown to be comparable to estimates from the general population20 and, as in our study, estimates from blood donors can be corrected for measured sampling biases. Few or no results were available from some geographical regions in Canada, notably the 3 territories. The variety of assays used across the included studies is another potential limitation, but the sensitivity and specificity of these assays was comparable.
Many of the challenges encountered in this study were a result of the lack of coordinated, ongoing serosurveillance capacity in Canada. We were able to bring together many estimates of seroprevalence to describe broad trajectories of population seroprevalence. However, routine serosurveillance — ideally with individual-level linkage to other data, such as testing and vaccination — would allow for a deeper understanding of the causal relationships between the timing and nature of immune system challenges and antibody levels in the population.21,22
Conclusion
Most people in Canada were infected with SARS-CoV-2 for the first time during the Omicron era, after previously being vaccinated. The highest rates of seropositivity from infection were seen in younger age groups and provinces in Western Canada. As a result, many people in Canada have hybrid immunity against SARS-CoV-2, but variations by age and geography and the potential for waning antibody levels suggest that public health policy and clinical decisions will need to be tailored to local patterns of population immunity.
Acknowledgements
The authors acknowledge the assistance of the COVID-19 Immunity Task Force Secretariat, all members of the research teams who carefully curated, processed and analyzed samples, and the volunteers and study participants who contributed invaluable samples for this seroprevalence study.
Footnotes
Competing interests: Maureen Anderson reports receiving a Saskatchewan Health Research Foundation Establishment Grant, in support of the present manuscript. Lesley Behl reports receving funding from the CITF via a research grant paid to the University of Saskatchewan, in support of the present manuscript. Patrick Brown reports receiving grant support from the CITF. Carmen Charlton reports receiving grant funding from Merck and support for attending meetings or travel from AMMI Canada. Karen Colwill reports receiving an honorarium for a presentation to the Ontario Society of Clinical Chemists. Dr. Colwill is also the vice president of communications for the Canadian National Proteomics Network. Tim Evans reports receiving support for the present manuscript from the CITF, and holds the role of its executive director. Anne-Claude Gingras reports receiving support for automated equipment for ELISA, housed at the Lunenfeld-Tanenbaum Research Institute (a facility supported by Canada Foundation for Innovation funding, the Ontario Government, Genome Canada and Ontario Genomics); support from the Canadian Institutes of Health Research (CIHR) for general lab operations; salary support as a Canada Research Chair (Tier 1) in functional proteomics; and from CITF and the Public Health Agency of Canada (PHAC) for assay calibration at Mount Sinai, all in support of the present manuscript. Dr. Gingras has had a contract with Providence Therapeutics (no consultation fees received), and has received grant funding from CIHR for several SARS-CoV-2 studies and from the Ontario Research Fund, outside of the present work. Dr. Gingras has served as the chair of the Institute Advisory Board of the CIHR Institute of Genetics and is a member and chair of the Human Health Therapeutics Division advisory board, National Research Council of Canada. Dr. Gingras is a member of the CITF working parties on testing and immunology, and is pillar lead of the Functional Genomics and Structure Function of CoVaRR-Net (all roles unpaid). Steven Drews reports receiving grants or contracts from CIHR and Alberta Innovates, consulting fees from Roche, support for attending meetings or travel from the Canadian Immunization Research Network and other support from Abbott. Jaspreet Jain reports receiving support from the CITF for the present manuscript. Prabhat Jha reports receiving grant support from the CITF for the Action to Beat Coronavirus study. Amanda Lang reports receiving funding from the CITF, in support of the present manuscript, for assay reagents and technologist salary. Dr. Lang has also received support from the CITF to attend a CITF meeting. Stephen Lee reports receiving funding from the CITF, in support of the present manuscript. Sheila O’Brien reports receiving payment (paid to Canadian Blood Services [CBS]) from the Government of Canada, and laboratory infrastructure from CBS, in support of the present manuscript. Chantale Pambrun reports receiving salary support from CBS, and study funding from PHAC. Olivia Oxlade is an employee of the CITF Secretariat. David Stephens reports receiving funds for a graduate student from the National Science and Engineering Research Council Emerging Infectious Disease Modelling, in support of the present manuscript. Hanna Swail reports receiving support from the CITF for the present manuscript. David Buckeridge reports receiving funding from PHAC, in support of the present manuscript. No other competing interests were declared.
This article has been peer reviewed.
Contributors: David Buckeridge, Bruce Mazer and Timothy Evans contributed to the conception and design of the work. Sheila O’Brien, Steven Drews, Carmen Charlton, Anne-Claude Gingras, Derek Stein, Prabhat Jha, Philip Awadalla, Maureen Anderson, Amanda Lang, Victoria Kirsh, Antoine Lewin, Marc-André Langlois, Stephen Lee, Kimberly Skead, Jamil Kanji, Graham Tipples, Paul Van Caeseele, Lesley Behl, Patrick Brown, Karen Colwill, Deena Hinshaw and Chantale Pambrun contributed to the acquisition and analysis of data. Tanya Murphy, Hanna Swail, David Stephens and David Buckeridge contributed to the interpretation of data. Bruce Mazer, David Buckeridge, Tanya Murphy, Jaspreet Jain, Hanna Swail and Olivia Oxlade drafted the manuscript. All of the authors revised the manuscript critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: These projects were supported by funding from the Public Health Agency of Canada, through the COVID-19 Immunity Task Force.
Data sharing: Data files are openly available under a CC BY-SA license through Borealis.
- Accepted July 4, 2023.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Dynamics of T cell responses to COVID-19 vaccines and breakthrough infection in people living with HIV receiving antiretroviral therapy
- Longitudinal Study on Seroprevalence and Immune Response to SARS-CoV-2 in a Population of Food and Retail Workers Through Transformation of ELISA Datasets
- Risk of hospital admission and death from first-ever SARS-CoV-2 infection by age group during the Delta and Omicron periods in British Columbia, Canada
More in this TOC Section
Similar Articles
Collections

