


Abstract
Background: Youth have reported worsening mental health during the COVID-19 pandemic. We sought to evaluate rates of pediatric acute care visits for self-harm during the pandemic according to age, sex and mental health service use.
Methods: We conducted a population-based, repeated cross-sectional study using linked health administrative data sets to measure monthly rates of emergency department visits and hospital admissions for self-harm among youth aged 10–17 years between Jan. 1, 2017, and June 30, 2022, in Ontario, Canada. We modelled expected rates of acute care visits for self-harm after the pandemic onset based on prepandemic rates. We reported relative differences between observed and expected monthly rates overall and by age group (10–13 yr and 14–17 yr), sex and mental health service use (new and continuing).
Results: In this population of about 1.3 million children and adolescents, rates of acute care visits for self-harm during the pandemic were higher than expected for emergency department visits (0.27/1000 population v. 0.21/1000 population; adjusted rate ratio [RR] 1.29, 95% confidence interval [CI] 1.19–1.39) and hospital admissions (0.74/10 000 population v. 0.43/10 000 population, adjusted RR 1.72, 95% CI 1.46–2.03). This increase was primarily observed among females. Rates of emergency department visits and hospital admissions for self-harm were higher than expected for both those aged 10–13 years and those aged 14–17 years, as well as for both those new to the mental health system and those already engaged in care.
Interpretation: Rates of acute care visits for self-harm among children and adolescents were higher than expected during the first 2 and a half years of the COVID-19 pandemic, particularly among females. These findings support the need for accessible and intensive prevention efforts and mental health supports in this population.
Self-harm among children and adolescents is a serious public health concern. A growing body of evidence, including from systematic reviews, suggests that during the COVID-19 pandemic, youth have reported higher levels of distress, increased symptoms of anxiety and depression1–4 and greater use of mental health services, 5 although data on whether this led to higher rates of self-harm (defined as the “intentional self-poisoning or self-injury, irrespective of type of motive or the extent of suicidal intent”6) in acute settings has varied.7 In the early months of the pandemic, national surveillance data of emergency department visits for suspected suicide attempts among youth in the United States showed an initial reduction in visits followed by a sustained increase through to 2021.8 Data from Ontario, Canada, however, showed a sustained decline in emergency department visits for self-harm among youth aged 14–24 years, through to June 2021.9 Recent meta-analyses of the later months of the pandemic, including predominantly high-income countries, showed a mounting trend in suicide-related behaviours among youth in the emergency department setting.10,11
Self-harm is a contemporaneous and objective indicator of child and adolescent mental health problems. It is more common than suicide and, therefore, leads to more reliable estimates of population trends; it is also a well-established predictor of suicide attempts among youth.12 When a child or adolescent presents acutely with self-harm, particularly as a first point of contact with health services, there is an important opportunity to engage them in timely and effective mental health care to mitigate suicide risk.
The interventions used for self-harm among children and adolescents in the acute setting, however, will vary according to the needs of the patient population. For example, during the pandemic, studies from several countries reported worsening mental health and increased mental health service use among adolescent females but not males.2,5,13–17 Middle schoolers (aged 10–13 yr) may have been particularly negatively affected by the pandemic.16,18 Middle school years are marked by factors that may make this group more susceptible to the deleterious effects of pandemic restrictions, such as extensive brain and cognitive development,19 immature impulse control,20 high relative importance of peers21 and a steep rise in the prevalence of symptoms of mental health disorders,22 including the onset of self-harm.6 Youth who used the emergency department as a first point of contact for mental health care during the pandemic, particularly for self-harm, are another group with a distinct profile of mental health needs.23
Understanding the patterns of pediatric self-harm during the pandemic among the early adolescent age group or according to history of mental health service use is essential to adapt mental health services to match need, allocate appropriate resources and develop targeted self-harm interventions and suicide prevention strategies. We sought to model expected rates of emergency department visits and hospital admissions for self-harm among children and adolescents during the COVID-19 pandemic, and to compare the observed and expected rates overall and by age, sex and mental health service use.
Methods
Study design and data sources
We conducted a population-based, repeated cross-sectional study of data from Ontario between Jan. 1, 2017, and June 30, 2022. In Ontario, physician visits, emergency department visits and hospital admissions are publicly funded. During the COVID-19 pandemic, Ontario had 3 province-wide emergency closures of schools, recreational programs, theatres, bars and restaurants and nonessential businesses (Mar. 17–July 24, 2020, Jan. 14–Feb. 19, 2021, and Apr. 8–June 9, 2021).24 School closures occurred March to June 2020, January to February 2021 (with periodic partial reopenings), April to June 2021 and in January 2022. For the 2021–2022 school year, families could choose in-person or remote learning.25
We used health administrative databases available at ICES, an independent nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement (Appendix 1, eTable 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.230127/tab-related-content). We used the Registered Persons Database (RPDB),26 the Ontario Health Insurance Plan (OHIP) database,27 the Canadian Institute for Health Information’s National Ambulatory Care Reporting System,28 the Discharge Abstract Database29 and the Ontario Mental Health Reporting System.30 Data held at ICES are complete and valid for primary discharge diagnoses, physician billing claims and sociodemographics.28–31 These data sets were linked using unique encoded identifiers and analyzed at ICES. We followed the relevant reporting guidelines, such as the Reporting of Studies Conducted Using Observational Routinely Collected health data (RECORD) statement.32,33
Study population
We included all children and adolescents aged 10–17 years residing in Ontario, Canada, and eligible for provincial health insurance on Jan. 1 of each year from 2017 to 2022. We excluded those with missing information for age and sex, non-Ontario residents and those not eligible for provincial insurance within 90 days of Jan. 1 of each year (Appendix 1, eTable 2). Using the RPDB, we identified each individual’s sex based on their health card (i.e., we were not able to identify gender). Henceforth, those identified as female on their health card will be referred to as females, and those identified as male will be referred to as males.
We identified youth as either new to mental health care, defined as those with no previous acute or outpatient mental health claims within 2 years before their monthly acute care presentation for self-harm (i.e., index date), or as continuing mental health care, defined as those with any acute or outpatient claim related to mental health (including but not limited to self-harm) in the 2 years before the index date. Outpatient mental health claims refer to physician billings associated with diagnostic codes that have been validated for use in Ontario health administrative data.27,34 Acute claims refer to broadly categorized diagnostic codes (F06–F99) from the Canadian version of the International Classification of Diseases, 10th Revision (ICD-10-CA)35 associated with hospital admissions and emergency department records, also used for performance measurement of the mental health system across Canada.36 We chose the 2-year period based on standards of clinical practice in Ontario (e.g., a consultation service to a patient by a specialist for the same diagnosis is eligible for payment only once every 2 years).37 If an individual was new to mental health care for 1 month and had self-harm visits in subsequent months, they would join the continuing mental health care group.
Identification of self-harm
We identified emergency department visits or hospital admissions for self-harm, defined by a discharge diagnosis of an ICD-10-CA diagnostic code for intentional self-harm (X60–X84, Y10–Y19 or Y28). These codes are used by the province of Ontario38 (and other provinces such as Manitoba39), the Public Health Agency of Canada,40 Statistics Canada,41 the Centers for Disease Control and Prevention42 and the World Health Organization43 for injury surveillance and have been validated in a study using physician diagnoses from emergency department visits (positive predictive value > 89.8%).44 We considered hospital admission as an indicator of self-harm severity.
We expressed monthly rates of emergency department visits and hospital admissions per 1000 or 10 000, respectively, of the Ontario population aged 10–17 years as of Jan. 1 of the corresponding study year (2017–2022). We calculated rates overall and by sex (male and female), age group (10–13 yr and 14–17 yr) and mental health service use (new and continuing). We grouped age into these 2 categories in keeping with the call to avoid combining pediatric age groups when making pandemic recommendations. 18 We calculated the number of unique youth with at least 1 visit for self-harm each month for emergency department visits and for hospital admissions, separately. We calculated monthly rates by including 1 visit per calendar month per individual. If an emergency department visit resulted in a hospital admission, we counted both an emergency department visit and an admission.
Covariates
We defined rurality using the definition from the Statistics Canada Postal Code Conversion File (version 2016)45 (community size ≤ 10 000). We obtained neighbourhood income quintile by linking this file with Census data.46
Statistical analysis
We used Poisson generalized estimating equations for count data to model pre-COVID-19 trends and estimated expected rates of emergency department visits and hospital admissions for self-harm during the pandemic period in the absence of restrictions, overall and by sociodemographic strata. The unit of analysis was age group–sex–month stratum. Full details of the modelling approach are in Appendix 1. We defined the prepandemic period as Jan. 1, 2017, to Feb. 28, 2020, and the COVID-19 pandemic as Mar. 1, 2020, to June 30, 2022. We calculated estimates of the relative change in post-onset event rates as an adjusted rate ratio (RR) of observed to expected rates and 95% confidence intervals (CIs) overall (as per our previous work5,47,48 and outlined in Appendix 1), as well as by sex, age group and mental health service use.
We conducted 2 sensitivity analyses. The first used prepandemic data from Jan. 1, 2013, until Feb. 28, 2020, and the second restricted data to the first emergency department visit or hospital admission during the study period for all youth. We performed analyses using SAS version 9.4 (SAS Institute).
Ethics approval
The use of these data was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board.
Results
Around 1.3 million children and adolescents aged 10–17 years living in Ontario were included in the annual population denominator, and demographics remained stable over the study period (Appendix 1, eTable 2 and eTable 3). Females constituted 48.7% of the population and the mean age was 13.5 (standard deviation 2.3) years. Ninety percent were living in urban areas, with proportions ranging from 18% to 23% across the 5 neighbourhood income quintiles. Figure 1 shows the observed and expected monthly rates of emergency department visits and hospital admissions for self-harm. Overall, the expected monthly rate of emergency department visits after the pandemic onset was 0.21 per 1000 population and the observed rate was 0.27 per 1000 population (adjusted RR 1.29, 95% CI 1.19–1.39) (Figure 1A and Appendix 1, eTable 4). Rates of hospital admission for self-harm were also higher than expected (0.74/10 000 observed v. 0.43/10 000 expected; adjusted RR 1.72, 95% CI 1.46–2.03) (Figure 1B and Appendix 1, eTable 4). The monthly rates of emergency department visits and hospital admissions remained higher than expected from January 2021 and July 2020, respectively, until June 2022 (Figure 1 and Appendix 1, eTable 4).

Observed and expected visit rates of (A) emergency department (ED) visits (per 1000 population) and (B) hospital admissions (per 10 000 population) for self-harm among children and adolescents aged 10–17 years from Jan. 1, 2017, to June 30, 2022, in Ontario, Canada. Vertical dashed line represents onset of COVID-19 pandemic restrictions.
Age and sex
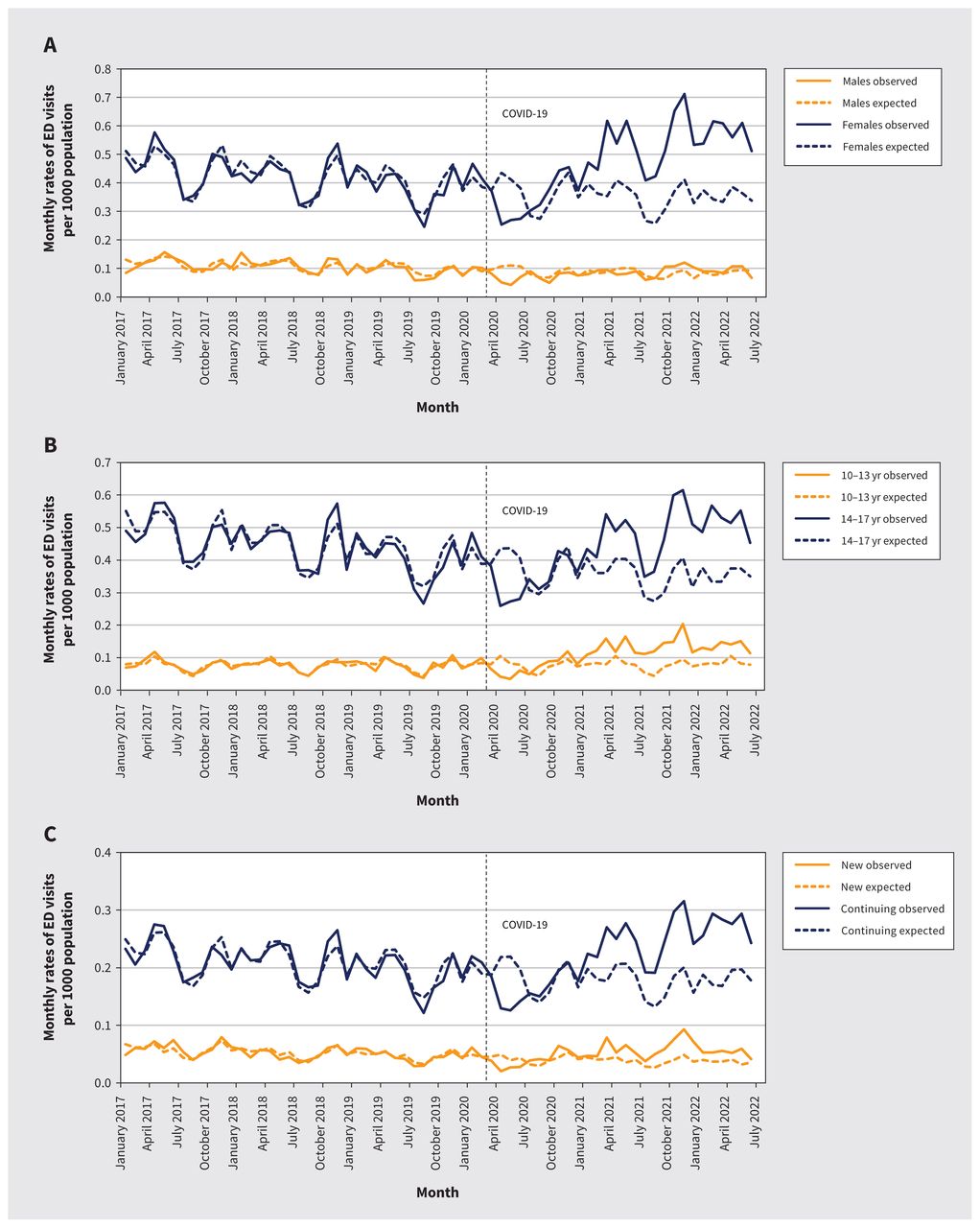
Rates of emergency department visits were higher than expected among females (0.48/1000 observed v. 0.35/1000 expected; adjusted RR 1.37, 95% CI 1.25–1.49) but not males (0.08/1000 observed v. 0.08/1000 expected; adjusted RR 0.99, 95% CI 0.88–1.11) (Figure 2A and Appendix 1, eTable 5). Rates of hospital admission were higher than expected among females (1.31/10 000 observed v. 0.73/10 000 expected; adjusted RR 1.80, 95% CI 1.48–2.18) and males (0.20/10 000 observed v. 0.15/10 000 expected; adjusted RR 1.34, 95% CI 1.19–1.50) (Figure 3A and Appendix 1, eTable 5).

Monthly rates of emergency department (ED) visits for self-harm from Jan. 1, 2017, to June 30, 2022, in Ontario, Canada, stratified by (A) sex (male and female), (B) age group (10–13 yr and 14–17 yr) and (C) mental health service use (new and continuing). Vertical dashed line represents onset of COVID-19 pandemic restrictions.

Monthly rates of hospital admissions for self-harm from Jan. 1, 2017, to June 30, 2022, in Ontario, Canada, stratified by (A) sex (male and female), (B) age group (10–13 yr and 14–17 yr) and (C) mental health service use (new and continuing). Vertical dashed line represents onset of COVID-19 pandemic restrictions.
Absolute rates of emergency department visits and hospital admissions were lower among youth aged 10–13 years than among those aged 14–17 years, although the relative increases in rates during the pandemic were highest in the younger group (Figure 2B, Figure 3B and Appendix 1, eTable 6).
Females aged 10–13 years had the largest relative increase in emergency department visits and hospital admissions during the pandemic (Figure 4, Figure 5 and Appendix 1, eTable 7).

Rate ratio (RR) of emergency department (ED) visits for self-harm during the COVID-19 pandemic by any, new, or continuing mental health care and age and sex group. Note: CI = confidence interval.

Rate ratio (RR) of hospital admissions for self-harm during the COVID-19 pandemic by any, new, or continuing mental health care and age and sex group. Note: CI = confidence interval. *Model could not converge because of small number of events.
New or continuing mental health service use
Among youth with new mental health service use, rates of emergency department visits (0.05/1000 observed v. 0.04/1000 expected; adjusted RR 1.35, 95% CI 1.16–1.57) and hospital admissions for self-harm were greater than expected during the pandemic (0.15/10 000 observed v. 0.07/10 000 expected; adjusted RR 2.02, 95% CI 1.58–2.59) (Figure 2C, Figure 3C and Appendix 1, eTable 8). Rates of emergency department visits and hospital admissions for self-harm were also greater than expected among youth with continuing mental health service use (0.22/1000 observed v. 0.18/1000 expected; adjusted RR 1.27, 95% CI 1.17–1.38; and 0.60/10 000 observed v. 0.36/10 000 expected; adjusted RR 1.65, 95% CI 1.32–2.07, respectively) (Figure 2C, Figure 3C and Appendix 1, eTable 8). Figure 4 and Figure 5 show the RRs of emergency department visits and hospital admissions for self-harm by any, new or continuing mental health care according to age group and sex.
Rurality and income quintiles
Across both urban and rural areas and high-and low-income neighbourhoods, youth had higher than expected rates of emergency department visits and hospital admissions for self-harm (Appendix 1, eTable 9 and eTable 10). The largest relative increase in emergency department visits occurred among youth living in urban areas (adjusted RR 1.30, 95% CI 1.18–1.42) and among those living in neighbourhoods of highest income quintile (adjusted RR 1.49, 95% CI 1.30–1.70). The largest relative increase in hospital admissions occurred among youth living in rural areas (adjusted RR 1.90, 95% CI 1.42–2.52) and those living in neighbourhoods of the lowest income quintile (adjusted RR 1.81, 95% CI 1.48–2.22).
Sensitivity analysis
The relative change in observed versus expected rates of hospital admissions was similar but less pronounced when we used monthly data from January 2013 rather than January 2017 (adjusted RR 1.25, 95% CI 1.12–1.39) (Appendix 1, eTable 11, and Appendix 2, Supplemental Figure 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.230127/tab-related-content). The observed and expected rates of emergency department visits did not differ significantly (adjusted RR 1.01, 95% CI 0.94–1.09), although, for both outcomes, the model fit was better with the more recent baseline.
When restricting analysis to the first emergency department visits and hospital admissions for self-harm, the relative change in observed versus expected rates was also similar to the main analysis (Appendix 1, eTable 12 and Appendix 3, Supplemental Figure 2, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.230127/tab-related-content).
Interpretation
In this population-based study of children and adolescents aged 10–17 years in Ontario, Canada, we observed a 29% increase in emergency department visits and a 72% increase in hospital admissions for self-harm during the COVID-19 pandemic, compared with expected rates. Although the absolute increase was small, the period with the greatest observed increase occurred in the latter half of the study period, well after the return of most in-person activities. Sensitivity analysis with a longer prepandemic period no longer showed a difference in the observed versus expected rates of emergency department visits, but the overall adjusted RR for hospital admissions was significant, which speaks to the robustness of this particular finding. Furthermore, the monthly rates of emergency department visits have been consistently higher than expected since March 2021. We observed marked sex-and age-specific patterns in acute care presentations for self-harm, wherein rates of emergency department visits and hospital admissions were higher than expected among females, especially those aged 10–13 years, a finding not observed among males of similar age. Younger adolescent females also constituted the largest group of new mental health service users accessing acute care for self-harm, with a sustained increase in hospital admissions from as early as the spring of 2020.
The increase in acute care visits for self-harm is consistent with data from the US8 and France49 but differs from the decline in emergency department visits for self-harm among older adolescents and young adults in Ontario during the first 15 months of the pandemic that was reported previously.9 Beyond differing methods and a longer follow-up period, the difference may be partly owing to the younger cohort in our study, who have less-developed coping strategies50,51 and who experienced one of the longest pandemic-related school closures in North America.25,52,53 Studies cannot feasibly evaluate the causal link between pandemic restrictions and self-harm among children and adolescents, 54 and many factors are at play,55 but findings may reflect the prolonged and cumulative effects of pandemic-related stressors on this younger age group such as social isolation, loss of routines, missed milestones, changing learning environments, familial stress, inadequately treated psychiatric conditions, substance misuse or changing patterns of mental health service use at a critical point in their developmental trajectory.1,53,56 Pandemic-related disruptions —such as limited access to primary care and community mental health services, staff absenteeism and redeployment of allied health professionals — are other possible contributors.57 It is unclear if this trend will persist beyond 2022, but findings from the first 2 and a half years of the pandemic reflect the complexities and long-term pandemic-related stress among children and adolescents.
The patterns of self-harm observed among adolescents echo previous findings from Canada,5 the US,8,58 Australia59 and other countries,16,60,61 and indicate that adolescent females may have been disproportionately affected by the pandemic.13–17,62 Although more research is needed, sex-and gender-specific stressors may be associated with the pandemic such as a differential or gendered response to less in-person contact with peers and social networks,63 cessation of in-person mental health support services, 60 more time on social media64,65 — which may present more opportunity for social comparison66–68 — and access to online communities that perpetuate self-harm contagion.68–71
Findings from this study should be interpreted in the context of well-established sex differences in psychiatric epidemiology among youth, including the preponderance of depression,72–74 higher reported prevalence of self-harm75,76 and more suicide attempts and mental health service use among adolescent females,77,78 all of which were trending upward before the pandemic.79–85 Indeed, younger females were the largest group of new users of acute mental health services in this study, which speaks to their baseline vulnerability. Similarly, older adolescent females with past or current use of mental health services, and therefore at higher risk of self-harm, had the largest increase in hospital admissions, which suggests severity of pathology. Taken together, the interaction of pandemic-associated stress with pre-existing risk factors could have shifted the tendency toward self-harm among young females. Lower rates of acute self-harm among adolescent males may not imply less need for mental health support. Males exhibit less health care-seeking behaviour than females,86 especially for mental health difficulty.87 Adolescent males may use coping mechanisms with less potential for a hospital visit, such as avoidance or distraction with video games,88,89 or reward-seeking behaviour with gambling.90,91
Limitations
Although we adjusted for several important covariates, residual confounding through unmeasured factors, such as family or interpersonal conflict, may have contributed to the observed results. This study also does not capture the community prevalence of self-harm that did not require acute hospital-based care92 and likely underestimates the extent of the problem. Erroneous coding of intentional self-harm as unintentional may have also contributed to underestimates of self-harm.93 Although sensitivity analysis suggested that subsequent visits did not inflate findings, this study was not designed to focus on frequent users of acute care for self-harm; this is a high-needs subgroup that merits targeted study. We also did not explore patterns of acute mental health service use for self-harm over the pandemic according to diagnostic group. Clinical thresholds for hospital admission for self-harm could have varied depending on the pandemic wave and hospital-specific factors. Data on race and ethnicity were not available in existing data sets, which precluded conclusions related to these variables. Finally, this study described data until June 2022; therefore, longer-term trends have not yet been studied.
Conclusion
We have shown a large and sustained increase above expected levels in presentations to hospital for self-harm by children and adolescents during the pandemic, particularly among younger females. The unabated demand for acute mental health services for self-harm among youth suggests lasting effects of the pandemic and continued under-treatment of mental distress in this population, despite the widespread lifting of pandemic restrictions. Beyond the pandemic, it will be important to understand the factors driving the observed upward trend in self-harm among youth. Long-term suicide prevention strategies among youth should be age-, sex-and gender-specific; include upstream interventions; and target pandemic-associated stressors. In the short term, accessible and intensive mental health supports are needed for this segment of the pediatric population.
Acknowledgement
The authors thank the Toronto Community Health Profiles Partnership for providing access to the Ontario Marginalization Index.
Footnotes
Competing interests: Rachel Mitchell reports receiving grants from the American Foundation for Suicide Prevention, the TD Pooler Fund and the Sunnybrook Foundation, as well as an Academic Scholar Award from the Department of Psychiatry at Sunnybrook Health Sciences Centre and the University of Toronto and an honourarium from Medscape. Eyal Cohen is a member of the Committee to Evaluate Drugs. Rachel Strauss reports consulting fees from Canadian Doctors for Prevention from Guns. Simone Vigod reports receiving authorship royalties from UpToDate. Kimberly Moran receives salary support from the Ontario College of Family Physicians. Astrid Guttmann reports receiving grants from the Canadian Institutes for Health Research. Paul Kurdyak is Vice President, Clinical at the Mental Health and Addictions Centre of Excellence at Ontario Health. Natasha Saunders reports receiving grants from the Canadian Institutes for Health Research, the Ontario Ministry of Health, the Centre for Addiction and Mental Health and The Hospital for Sick Children, as well as personal fees from the BMJ Group for her role as associate editor for the Archives of Diseases in Childhood. She is a member of the Canadian Paediatric Society Mental Health and Developmental Disabilities committee. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Rachel Mitchell, Alene Toulany, Longdi Fu, Therese Stukel, Rachel Strauss and Natasha Saunders conceptualized and designed the study. Hannah Chung had access to and analyzed the data. All of the authors contributed to data interpretation. Rachel Mitchell and Natasha Saunders drafted the initial manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MHLTC). This study also received funding from the Canadian Institutes of Health Research (UIP-178845), awarded to Natasha Saunders and Alene Toulany. This document used data adapted from the Statistics Canada Postal Code Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from Canada Post Corporation and Statistics Canada.
Data sharing: The data sets from this study are held securely in coded form at ICES. Data-sharing agreements prohibit ICES from making the data sets publicly available, but access may be granted to those who meet pre-specified criteria for confidential access, available at www.ices.on.ca/DAS. The complete data set creation plan, and underlying analytic code are available from the authors upon request, understanding that the programs may rely upon coding templates or macros unique to ICES.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and Ministry of Long-Term Care (MLTC). The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOH or MLTC is intended or should be inferred. This document used data adapted from the Statistics Canada Postal Code Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from Canada Post Corporation and Statistics Canada. Parts of this material are based on data and information compiled and provided by the MOH and Canadian Institute for Health Information (CIHI). The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
- Accepted July 14, 2023.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

