


Abstract
BACKGROUND: Diabetes mellitus is an established health concern in First Nations communities and is associated with complex influences of colonization. This study, a partnership between First Nations and academic researchers, was undertaken to determine patterns of diabetes prevalence, incidence and mortality in Ontario.
METHODS: Using health services and population data from Ontario for 1995 to 2014, linked with the federal Indian Register, we calculated age- and sex-adjusted annual estimates of diabetes prevalence, incidence and mortality for First Nations people (living within and outside First Nations communities) and other people in Ontario. We also examined age- and sex-specific crude diabetes prevalence.
RESULTS: Between 1995 and 2014, the prevalence of diabetes increased and the incidence decreased somewhat in all populations. Both prevalence and incidence were substantially higher among First Nations people than among other people in Ontario. In particular, First Nations women had higher prevalence than other women (4.2% v. 1.6% for ages 20–34 yr and 17.6% v. 6.0% for ages 35–49 yr). The lifetime risk of diabetes was higher among First Nations people than among other people in Ontario (57.0%, 95% confidence interval [CI] 56.3%–57.6% v. 44.5%, 95% CI 44.4%–44.6%). Over time, all-cause mortality for those with diabetes declined but remained consistently higher for First Nations people than for other people in Ontario.
INTERPRETATION: Diabetes is more common among First Nations people than among other people in Ontario, particularly at younger ages and in women. First Nations–led approaches to address the high prevalence of diabetes in younger First Nations women have the potential to improve metabolic health across generations.
Diabetes mellitus is an established health concern for First Nations in Canada1,2 and is associated with other chronic conditions, increased risk of death and higher health care use.3,4 Among First Nations people, the prevalence of diabetes is 3 to 5 times higher than in other populations.5,6 An estimated 8 in 10 First Nations people in Alberta will develop diabetes during their lifetime.5 In First Nations people, diabetes tends to occur at younger ages, with higher complication rates, than in the general population.5,7,8 A complex set of physical and social factors underlie these patterns,6 including the intergenerational impacts of ongoing colonial policy and resultant social, political, economic and cultural inequities.6,9,10
Current population-level, First Nations–specific information about diabetes rates, patterns and trends are not available and accessible to First Nations who might be able to inform and develop population approaches to prevent and manage diabetes.11 This study, a collaboration between academic researchers and researchers at Chiefs of Ontario, was undertaken to address this gap. The primary objectives were to determine overall population-level patterns of diabetes prevalence, incidence and mortality among First Nations people in Ontario over a 20-year period, from 1995 to 2014, and to describe the lifetime risk of diabetes for First Nations people in Ontario.
Methods
We have described elsewhere the details of our research partnership12 and our use of administrative health data at ICES.13,14 Briefly, we accessed health services and population data at ICES for the period Apr. 1, 1995, to Apr. 1, 2014. We included all individuals from the Registered Persons Database who were Ontario residents eligible for a health card, had contact with the health care system within the past 7 years and were 105 years of age or younger.
We identified First Nations people through a previous linkage of the federal Indian Register to the Registered Persons Database.15 This register includes all people registered with the federal government as a “Status Indian” under the Indian Act,16 regardless of whether or not they live in a First Nation community (“Indian Reserve”16).
Diabetes status was determined using the Ontario Diabetes Database, which cannot distinguish between type 1 and type 2 diabetes and excludes data on patients with gestational diabetes. This method of identifying people with diabetes in Ontario health services databases has been validated against primary care health records and has a sensitivity of 86% and a specificity of 97%.17
We estimated the annual crude and age- and sex-standardized prevalence of diabetes from 1995 to 2014 among First Nations people and other people in Ontario. The numerators included individuals who were alive and who were identified (using the Ontario Diabetes Database) as having a diagnosis of diabetes by the end of each year. We stratified the data as to whether or not the people lived within a First Nation community using a combination of residence and postal codes for each year from 2001 onward, because the reliability of geographic data was limited before then.
We examined the trends in crude prevalence stratified by age and sex simultaneously to explore the effect of the interaction of age and sex on the prevalence of diabetes for First Nations and other people in Ontario. For this, and all age-stratified analyses, we grouped ages 0 to 19 years, 20 to 34 years, 35 to 49 years, 50 to 64 years, 65 to 74 years, and 75 years or older. Although these age groups are generally 15-year age categories, the category for 0 to 19 years was chosen to ensure that we could look at children and youth separately from adults. For the oldest age groups, there were too few people aged 80 or older to maintain the 15-year age groupings, so 75 or older was used as an alternative grouping.
Similarly, we calculated annual crude and age- and sex-standardized incidence of diabetes for 1995 to 2014 for First Nations people and other people in Ontario. We included all newly diagnosed cases in a particular year in the numerators and all individuals exposed to risk who had no previous diagnosis of diabetes and who were alive at the end of the fiscal year in the denominators. We examined the annual incidence separately for First Nations people living within and outside First Nations communities. We also calculated age- and sex-specific crude estimates.
We conducted a sensitivity analysis to assess the effect of excluding those who were not alive at the end of the study period. For each of the groups, we compared the age- and sex-standardized prevalence and incidence between those who remained alive in 2014 and those who were alive plus those who died.
To estimate mortality among those with diabetes, we used the Registered Persons Database to identify those with diabetes who died from all causes in a given year and compared the age-and sex-standardized rates for First Nations and other people in Ontario. For all age- and sex-standardized rates, we used direct standardization based on the 2001 Ontario census population and assumed a gamma distribution for the observed standardized rates to estimate 95% confidence intervals (CIs),18 to adjust for the differences in population distribution between populations and over time.
To estimate the lifetime risk of diabetes in First Nations people and other people in Ontario, we calculated age-specific incidence using 5-year age categories from 1995 to 2014. We adjusted for the competing risk of death to estimate the sex-specific risk of diabetes occurring at some point throughout a person’s life, in an approach parallel to the one used by Turin and colleagues5 in Alberta and using a published Practical Incidence Estimators SAS macro.19 We calculated risk ratios between First Nations and other people in Ontario in each age category.
All analyses were conducted using SAS Enterprise Guide version 7.1 (SAS Institute Inc.).
Ethics approval
In addition to adherence to Ontario First Nations data governance processes, including review and approval by the Data Governance Committee, our project was reviewed and approved by the Research Ethics Boards at Queen’s University and Laurentian University.
Results
The 2014 age and sex distribution for First Nations people living within and outside First Nations communities and other people in Ontario is summarized in Table 1. On average, First Nations people were younger than other people in Ontario. The age and sex profile of First Nations people was similar for those living within and outside First Nations communities.
Demographic characteristics of First Nations people (living within and outside First Nations communities) and other people in Ontario, 2014
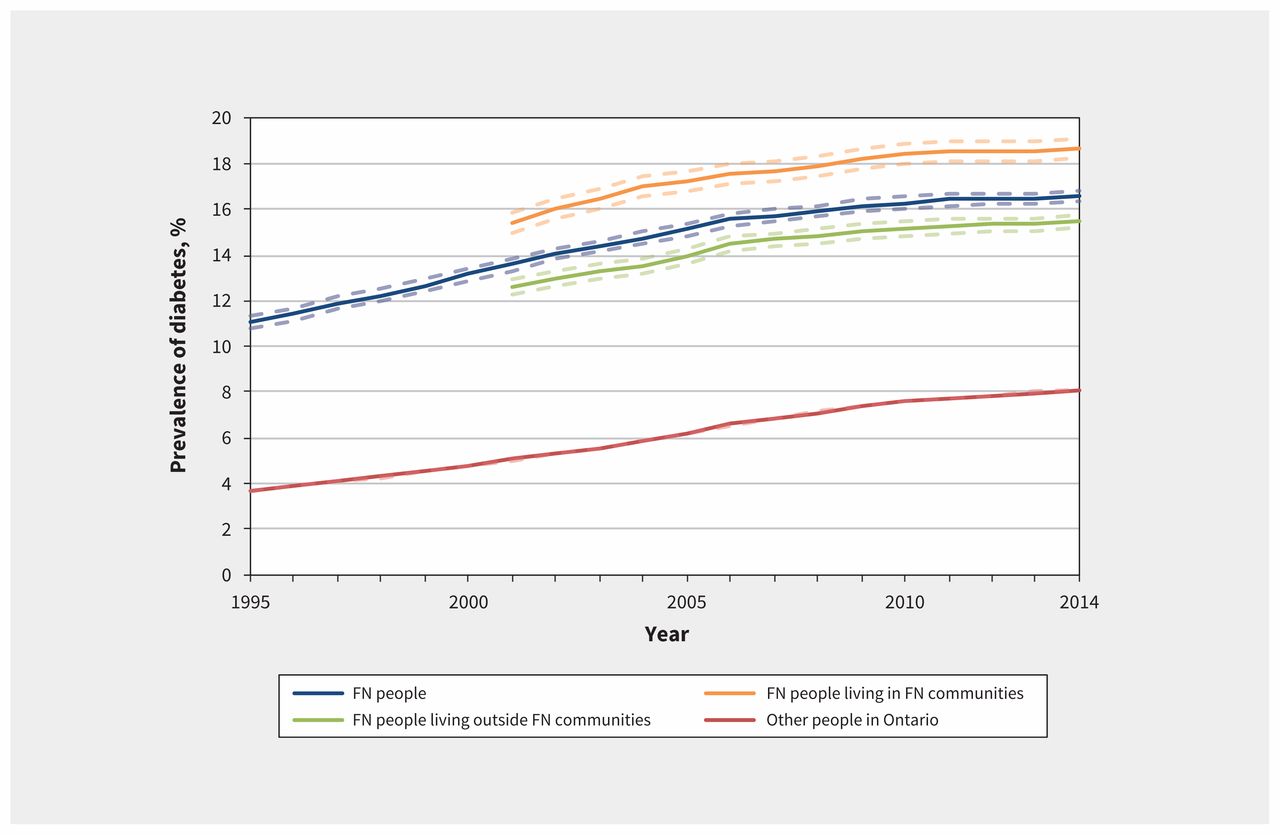
The prevalence of diabetes was substantially higher among First Nations people than among other people in Ontario (Figure 1). The annual age- and sex-standardized prevalence of diabetes increased for all study populations over time. The adjusted prevalence for First Nations people rose from 11.1% (95% CI 10.8%–11.3%) in 1995 to 16.6% (95% CI 16.4%–16.8%) in 2014. Prevalence was highest among those living in First Nations communities, rising from 15.4% (95% CI 15.0%–15.9%) in 2001 to 18.7% (95% CI 18.3%–19.1%) in 2014.

Age- and sex-standardized prevalence of diabetes mellitus among First Nations (FN) people living within and outside First Nations communities and among other people in Ontario, 1995–2014. Data on residence within or outside First Nations communities were available from 2001 onward. Note: Dashed lines represent 95% confidence intervals.
The annual age- and sex-standardized incidence of diabetes among First Nations people in Ontario decreased from 10.7 per 1000 people in 2001 to 8.0 per 1000 people in 2014 (Figure 2). Despite this 25% decrease, the age- and sex-standardized rate of new cases of diabetes remained higher among First Nations people than other people in Ontario, for whom incidence initially rose from 0.55% to 0.69% between 2001 and 2006 and then gradually declined to 0.49% in 2014. Over time, the incidence of diabetes was similar for First Nations people living within and outside First Nations communities (Figure 2).

Age- and sex-standardized incidence of diabetes mellitus among First Nations (FN) people living within or outside First Nations communities and among other people in Ontario, 1995–2014. Data on residence within or outside of First Nations communities were available from 2001 onward. Note: Dashed lines represent 95% confidence intervals.
We found consistent patterns from 1995 to 2014 for the effect of the interaction of age and sex on the crude prevalence and incidence estimates. Thus, for 2014, our most recent year of data, we displayed the crude prevalence and incidence estimates by age and sex simultaneously (Figure 3). Younger First Nations women had a more than 2.5-fold higher prevalence than other women (4.2% v. 1.6% for ages 20–34 yr; 17.6% v. 6.0% for ages 35–49 yr). Likewise, those same groups of First Nations women had a 2.8-fold higher incidence than other women in Ontario (5.8 v. 2.1 new cases per 1000 for ages 20–34 yr; 15.1 v. 5.3 new cases per 1000 for ages 35–49 yr). Among First Nations people, the age-adjusted incidence of diabetes was similar for men and women; however, among other people in Ontario, the incidence was higher for men.

Age- and sex-specific prevalence (A) and incidence (B) of diabetes mellitus among First Nations (FN) people living within or outside First Nations communities and among other people in Ontario, 2014.
Figure 4 displays the cumulative incidence of diabetes among First Nations people and other people in Ontario. The overall lifetime risk of diabetes was 57.0% (95% CI 56.3%–57.6%) for First Nations people and 44.5% (95% CI 44.4%–44.6%) for other people. The observed divergence of the curves with age is the result of high ratios of the cumulative incidence observed between ages 20 and 50, with a peak at age 30, when cumulative diabetes incidence was 2.9 times higher among First Nations people than among other people in Ontario (4.3% [95% CI 4.1%–4.5%] v. 1.5% [95% CI 1.5%–1.5%]).

Lifetime risk of diabetes mellitus among First Nations people and other people in Ontario by age, 1995–2014. Note: Dotted lines represent 95% confidence intervals.
As shown in Figure 5, although mortality rates for those with diabetes decreased from 1995 to 2014 in both First Nations people and other people in Ontario, they remained higher for First Nations people, particularly since 2001. In 2014, the all-cause mortality rate among First Nations people with diabetes was 33.32 per 1000 people, compared with 25.43 deaths per 1000 people among other people with diabetes in Ontario.

Age- and sex-standardized all-cause mortality rates among First Nations (FN) people and other people in Ontario with diabetes mellitus, 1995–2014. Data on residence within or outside First Nations communities were available from 2001 onward. Note: Dashed lines represent 95% confidence intervals.
The sensitivity analysis showed that excluding the 94 439 individuals who died during the study period did not affect the estimates of prevalence and incidence for the study groups.
Interpretation
We found that First Nations people continue to experience higher prevalence of diabetes than other people in Ontario, which is consistent with previous research. Although previous estimates have reported prevalence as being 3 to 5 times higher in First Nations populations,5,20 we observed a narrowing of this gap, from 3 to 2 times, over the period from 1995 to 2014 in Ontario. This finding is likely due, in part, to an observed 25% decline in the incidence of diabetes among First Nations people over the study period. We also observed a decrease in incidence for other people in Ontario, beginning around 2007. This drop in diabetes incidence has been seen in other provinces of Canada and in the United States.21 While these findings represent promising progress, and may indicate real declines in the risk of diabetes, the declines in incidence do not track with declining prevalence of diabetes risk factors13 and may be an artifact of changing diagnostic criteria or screening practices.22
Diabetes prevalence and incidence among First Nations people were particularly higher than among other people in Ontario for younger ages and for women. The greatest relative difference in prevalence occurred among those aged 35 to 49 years, whereby First Nations people had a nearly threefold higher prevalence. In contrast to the situation for other people in Ontario, with men having higher rates of diabetes than women, we saw the opposite trend among First Nations people. Consistent with previous findings,7,8,23 First Nations women had higher prevalence than men and similar incidence. The algorithm used in this study did not include gestational diabetes; therefore, the difference cannot be attributed to the documented increase in prevalence of diabetes complicating the pregnancies of First Nations women.24,25 This combination of diabetes occurring at younger ages and more commonly in women raises concerns about the high prevalence of diabetes in women of child-bearing age.26 These concerns have implications for metabolic health across generations, given that children born to mothers with pre-existing diabetes are more likely to have type 2 diabetes, adiposity and lipid abnormalities.24,25,27,28 In addition, we explored outcomes for diabetes in pregnancy in another study13 and found that the birth outcomes were more strongly affected by the presence of diabetes for First Nations women than for other women in Ontario.
First Nations people living within First Nations communities had higher prevalence of diabetes, although the incidence of diabetes was similar among those living within and outside First Nations communities. In a previous study of 13 First Nations communities in Alberta, communities with higher knowledge of Indigenous language had significantly lower diabetes prevalence.29 In contrast, Dyck and colleagues30 found that individual-level cultural disruption was not predictive of diabetes risk and that Cree language use was not a protective factor. These complex interactions among land, culture, environment, community, colonial disruption and risk of diabetes are best understood using a framework based on Indigenous determinants of health.10
While mortality rates have been decreasing among First Nations people in Ontario, in Canada and around the world,31 we found that all-cause mortality rates for those with diabetes remained higher among First Nations people than among other people in Ontario. Higher mortality rates have been reported for other Indigenous populations in Canada32 and internationally.33 Avoidable mortality, that is, deaths that could potentially have been avoided through either prevention or treatment (including prevention or treatment of diabetes), has been shown to be significantly higher among First Nations people in Canada than the rest of the population.32
Limitations
To identify people with diabetes, we relied on the Ontario Diabetes Database, which requires that a diagnosis of diabetes be recorded in either a hospital admission record or physician billing claims. Although this algorithm has high sensitivity and specificity for diabetes in the general population,17 its validity for First Nations populations has not been assessed. Diabetes diagnosed in individuals who receive primary care from other than fee-for-service billing physicians (including through Aboriginal Health Access Centres, Community Health Centres and nursing stations) may be missed, because such care encounters do not generate an Ontario Health Insurance Plan claim. Use of this database would thus result in underestimation of the prevalence and incidence of diabetes. However, the proportion of the First Nations population living within the service areas of the Aboriginal Health Access Centres and nursing stations is relatively small, so underestimation of diabetes would be moderate. The algorithm also does not distinguish between types 1 and 2 diabetes. Most people with diabetes mellitus in the First Nations population are likely to have type 2 disease, but the proportion of diabetes accounted for by type 2 in specific subgroups cannot be confirmed from the data available. An additional limitation of the Ontario Diabetes Database is that it did not allow us to look at trends in prediabetes, which would require access to laboratory data.
Our decision to limit our prevalence and incidence calculations to those who survived the fiscal year may have resulted in a slight underestimation for each group. However, we conducted a sensitivity analysis and found negligible impact of this decision on our conclusions. To determine whether individuals lived in First Nations communities, we relied on the availability of a residence code recorded in hospital or emergency department data. Where such a code was not available, we estimated location using the postal code that was registered in the person’s health card address. This information may be outdated, given the high mobility of First Nations people.34,35 In addition, the Registered Persons Database contains information for a small number of individuals who are deceased or no longer living in Ontario; as such, this database likely underestimates mortality.
Conclusion
The prevalence of diabetes among First Nations people continues to rise and is persistently higher than among other people in Ontario. However, with fewer newly diagnosed cases of diabetes in First Nations people over time, the growth in prevalence is slowing, and the gap in prevalence of diabetes between First Nations people and other people in Ontario has narrowed. Diabetes in First Nations people occurs at younger ages and more often in women, compared with other people in the province. As such, it is particularly important to address diabetes in women of reproductive age, because of the potential generational impacts on metabolic health. Furthermore, efforts to prevent and manage diabetes in First Nations people requires a grounded understanding of the determinants of health that affect First Nations in Canada, including the ongoing, intergenerational impacts of colonial policy associated with social, political, economic and cultural inequities.
Acknowledgements
The authors’ partner through the early design, implementation and final dissemination phases of this project was the Chiefs of Ontario. Their many member contributions were key to the content and quality of the project. The authors also acknowledge the members of the Patient Advisory Committee for providing insightful and thoughtful input; their advice made an important contribution in shaping the work. For a complete list of the individual members of the committee, see the full report (cited as reference 13 in the article). The authors would also like to thank Robyn Rowe, Sue Schultz, Rahim Moineddin and Rebecca Griffiths for their contributions. They also acknowledge Tanvir Turin Chowdhury for assistance in calculating lifetime risk of diabetes.
Footnotes
Visual abstract available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.190836/-/DC1
Competing interests: Michael Green received consulting income from the First Nations and Inuit Health Branch of Health Canada for work related to Jordan’s Principle, outside the scope of this study. No other competing interests were declared.
This article has been peer reviewed.
Contributors: All of the authors made substantial contributions to the conception and design of the study. Shahriar Khan conducted the analysis. The authors met to discuss the conceptual themes for this manuscript, and Jennifer Walker and Morgan Slater produced the initial draft. All of the authors were closely involved with reviewing early drafts, made critical revisions throughout all stages, approved the final version to be published and agreed to be accountable for the work.
Funding: This study was supported by an Ontario SPOR Support Unit IMPACT Award. Additional support was provided by Michael Green through the Brian Hennen Chair in Family Medicine and by Jennifer Walker through a Tier 2 Canada Research Chair in Indigenous Health and through ICES.
Data sharing: The data used in this study are held at ICES and are not available for sharing from the authors. Contact ICES (www.ices.on.ca) for more information.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information, Cancer Care Ontario and the Ontario MOHLTC. The analyses, conclusions, opinions and statements expressed in this paper are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
- Accepted December 12, 2019.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Characterizing the cascade of care for hepatitis C virus infection among Status First Nations peoples in Ontario: a retrospective cohort study
- Correction to "Diabetes prevalence, incidence and mortality in First Nations and other people in Ontario, 1995-2014: a population-based study using linked administrative data"
- Monitoring, treatment and control of blood glucose and lipids in Ontario First Nations people with diabetes
- Use of the health care system by Ontario First Nations people with diabetes: a population-based study
More in this TOC Section
Similar Articles
Collections

