


Author video summary at www.cmaj.ca/lookup/doi/10.1503/cmaj.220525/tab-related-content
We prepared to anesthetize an 83-year-old, 75-kg man with an unstable cervical vertebra 5 (C5) spine fracture for a posterior cervical decompression and fusion. He was neurologically intact, wearing a hard cervical collar, and had fasted for more than 12 hours. Assuming an “empty” stomach, we planned to intubate using an asleep fibre optic technique to minimize neck movement during airway manipulation. However, during the preoperative evaluation, the patient reported nausea.
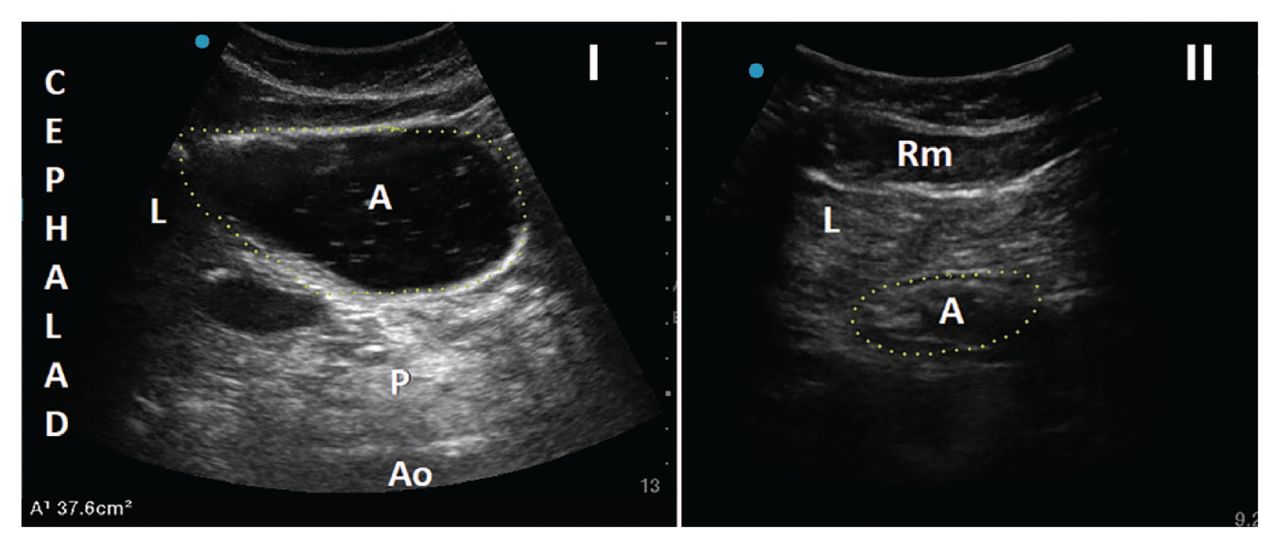
We performed a gastric ultrasound examination using a previously described protocol.1 We used a Sonosite Edge portable ultrasound unit and a curvilinear transducer to identify the antrum in a sagittal plane in the epigastric area. The patient’s antrum appeared grossly distended with hypoechoic fluid content in both supine and right lateral decubitus positions (Grade 2 antrum)1 with an estimated volume of more than 400 mL (Figure 1-I and Appendix 1, supplementary video 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220525/tab-related-content). We drained 450 mL of fluid from his stomach using a nasogastric tube. Repeat examination confirmed an “empty stomach” (Grade 0 antrum) with an estimated volume of 10 mL (Figure 1-II and Appendix 2, supplementary video 2, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220525/tab-related-content). We then performed a standard intravenous anesthetic induction and fibre optic endotracheal intubation with no complications.

Sonographic images of the antrum of an 83-year-old man’s stomach in the right lateral decubitus position. (I) The antrum appears grossly distended with clear fluid (hypoechoic content); the cross-sectional area of 37 cm2 corresponds to a volume > 400 mL. (II) Empty antrum after nasogastric suction; the cross-sectional area of 5.7 cm2 corresponds to a volume of about 10 mL. Note: A = antrum, Ao = aorta, L = liver, p = pancreas, Rm = rectus muscle. Used with permission from Dr. Perlas Fontana Medicine Professional Corporation.
Aspiration of gastric contents is a serious anesthetic complication that can cause considerable morbidity and mortality.2,3 The frequency of aspiration for elective surgical patients who are fasting is 1:3000, but it can be as high as 30% in patients with severe trauma who require intubation.2 Risk factors include urgent or emergency surgery, bowel obstruction, labour, diabetes and renal failure.4 Interventions that may decrease the risk include fasting preoperatively, evacuation of gastric content via a nasogastric tube and a rapid sequence induction of anesthesia, followed by endotracheal intubation.5 Point-of-care gastric ultrasound is a low-cost, noninvasive and relatively easy bedside intervention with the potential to decrease aspiration risk when the volume of gastric content is uncertain, based on clinical information.
Videos showing a distended antrum in the right lateral decubitus with an estimated gastric volume > 400 mL of clear fluid, then an empty antrum after decompression via a nasogastric tube, are available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220525/tab-related-content
Footnotes
Competing interests: Anahi Perlas is a member of the American Society of Anesthesiologists Editorial Board on point-of-care ultrasound and the executive editor for Regional Anesthesia and Pain Medicine. No other competing interests were declared.
This article has been peer reviewed.
The authors have obtained patient consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

