


Although data on race and ethnicity are not routinely collected in health data sets and disease registries in Canada, a few data linkage studies have shown that the burden of breast, colorectal, prostate and pancreatic cancers is higher in Black patients than in white patients in Canada.
Black patients are faced with several barriers that can threaten access to novel oncologic advances, such as cancer screening, molecular testing, breakthrough targeted therapies and enrolment in clinical trials.
Routine collection of race and ethnicity data in Canada can guide epidemiologists, clinical trial developers and health care providers to design targeted interventions and help equalize access to cancer care.
Proven measures to improve trial and screening enrolment include employing a diverse health care team, using multilingual lay health educators and being sensitive to the sources and types of media some Black patients are using for their health information.
Cancer survival is improving in Canada owing to earlier detection and treatment advances. Despite publicly funded health care in Canada, access inequities can prevent Black patients from achieving the full benefits of these advances in care. According to the most recent analysis of Canadian Cancer Registry (CCR) data from 2006 to 2016, linked to race and ethnicity data from the Canadian Census, mortality from breast, colorectal, prostate and pancreatic cancers is higher in Black patients than in white patients.1 In general, however, the impact of ethnicity on cancer incidence and mortality is infrequently studied in Canada because Canadian registries do not routinely collect race and ethnicity data, unlike databases in the United Kingdom and the United States. Studies from the UK have shown that Black African and Caribbean men are more likely to develop prostate cancer, and survival is prolonged when access to cancer treatment is equalized.2 We examine key areas where access inequities exist in Canada, and discuss mechanisms to improve access to cancer care for Black patients, based on a targeted search for evidence as outlined in Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.212076/tab-related-content.
What is known about gaps in access to care for Black patients with cancer in Canada?
In Canada, a lack of routine collection of race-based data by provincial and territorial cancer registries limits our understanding of how access to various cancer services affects racialized populations. Despite this limitation, some studies have linked Census data to provincial registry data to learn how ethnicity affects cancer screening, incidence and mortality.1 Some provincial databases also use geography and socioeconomic status as imperfect surrogates for race and ethnicity. These approaches are inadequate and Canadian data on how race and ethnicity affect access to cancer clinical trials, hematopoietic stem cell transplantation (HSCT) and uptake of personalized medicine are lacking.
Detecting cancer at an early stage leads to better outcomes, including reduced morbidity and mortality, and improved survival.3 Population-based screening programs for breast, cervical and colorectal cancers have been implemented across Canada, but Black and immigrant populations are disproportionately underrepresented in regular screening.4 A population study of immigrant women in Ontario found that lack of cervical cancer screening was significantly associated with not having a female physician, not having a primary care provider at all, or coming from low-income households.5 Thus, Black patients may experience additional barriers to cancer screening programs, and these barriers could limit uptake of screening services. Clinical trials study novel tests and treatments for cancer to establish standards of care. Research that results in new standards of care should be representative of the population who will benefit, and under-representation can threaten the external validity of results.
Clinical trials can also provide an opportunity to access breakthrough tests and treatments. The negative experiences of Black participants in the Tuskegee Syphilis Study introduced mistrust of health care systems. 6 Despite the international ethical codes that have been established in the past 50 years to prevent unethical research and combat institutional racism, ongoing public distrust can affect clinical trial enrolment, particularly in the Black population. In a Canadian pediatric study of enrolment in cancer clinical trials, Black youth were not found to have a lower enrolment rate, though low enrolment was observed among youth of Asian and Arab descent.7 Race has not been studied in clinical trial enrolment for the Canadian adult population as a whole. However, research from the US using cartographic mapping showed that areas with the highest density of Black people did not necessarily have high accrual of racialized patients, suggesting that distance was not a barrier to enrolment in clinical trials.8
Hematopoietic stem cell transplantation offers life-saving therapy for many hematological cancers, but is a resource-intensive procedure that is offered only at specialized centres. Differential access has been described, with lower rates of HSCT among Black patients.9,10 The impact of race on HSCT access has not been well studied in Canada, owing to minimal collection of race data, but 1 pediatric HSCT study in Canada showed no differences by race among children with acute lymphoblastic leukemia.11
Contemporary cancer care uses evidence to support the delivery of personalized medicine. For example, patients with advanced, EGFR-mutated lung cancer can receive targeted therapy with osimertinib, which is more effective and better tolerated than cytotoxic chemotherapy.12 Similarly, adjuvant treatment of early-stage breast cancer is reliant on genomic profiling of tumours with a 21-gene assay that informs the risk of recurrence and whether chemotherapy is warranted.13 In this era of molecular cancer treatment, inadequate access to molecular diagnostics limits treatment decision-making; as such, patients without access to molecular testing receive comparatively substandard care. Personalized cancer tests and treatments are increasingly costly, and timelines for provincial funding of these advances can be lengthy in Canada.14 Before provincial funding, personalized treatments could be accessed through special-access programs, insurance company coverage or patient out-of-pocket payment. The latter 2 methods can disproportionately expose Black patients to heavy financial burdens. Ezeife and colleagues15 previously showed that patients in Canada with no private insurance coverage experienced more financial toxicity, even in the context of publicly funded health care.
What could improve access to cancer care for Black patients?
For visible minorities and immigrant populations, approaches that have proven effective at enhancing screening uptake include cultural awareness training for health care providers, use of culturally focused media, use of multilingual health educators, and use of lay health educators and patient navigators.16 These techniques can also be applied to improve understanding, health literacy and adherence to cancer treatments. The American Society of Clinical Oncology endorses strategies to increase racial and ethnic diversity in clinical trials.17 The society recommends partnering with patients and community leaders to design and conduct clinical trials that focus on reducing barriers for racialized patients.17 Mutebi and colleagues8 examined models to enhance patient engagement in clinical trials in Africa. Key strategies that emerged included enhanced focus on how to manage fear to encourage clinical trial recruitment and how to build trust to retain clinical trial participants.
Access to cancer care is mediated by patient awareness and views on symptoms, diagnosis and treatment, which can be influenced by cultural background. Studies in the UK have shown that the development of culturally appropriate materials can help decrease stigma and taboos surrounding cancer diagnosis and treatment among racialized populations. For instance, treatment for prostate cancer can cause erectile dysfunction and urinary incontinence, and culturally mediated views of masculinity among Black men can negatively affect uptake of prostate cancer treatment.19 Increasing awareness and designing educational materials discussing these side effects can break the stigma to enhance communication between Black patients and their health care team. Jones and colleagues20 showed that culturally determined views also guided women’s understanding of breast cancer symptoms and likelihood of seeking medical attention in the UK. Although all Black women expressed uncertainty over breast awareness, and viewed themselves as low risk for developing breast cancer, first-generation, Black African women experienced the greatest delays in breast cancer diagnosis.
Diversity exists within the Black community, and research increasingly suggests that the sources and types of health information are important to highly educated Black patients and Black immigrants who have experienced acculturation. Previous data from Haitian immigrants showed that an inverse relationship exists between educational attainment and the use of multiple sources of media for health information.21 Highly educated patients were more likely to use a single source for health information such as the Internet or their health care provider, while patients with lower educational attainment were more likely to rely on multiple sources within their social networks (i.e., friends, family and religious organizations) to inform their health behaviours.
What steps should Canada’s health systems take to improve access to cancer screening and care for Black people?
Routine collection of race and ethnicity cancer data
Race and ethnicity data have historically been considered sensitive to collect in Canada because care must be taken to ensure that these data are collected in the most ethical and meaningful way. In addition, researchers collecting and analyzing these data must have an intrinsic understanding of disparities, and commit to eliminating the disparities that are discovered. Although extensive race and ethnicity data related to cancer are collected and reported in the US and the UK, these data cannot be generalized to the Canadian population. Canada has a different racial and demographic composition than these other jurisdictions.22 Unlike the UK health care system, where the private and public systems coexist in parallel, Canada’s health care systems aim to promote equal access of health services to the population. In reality, use of health services differs substantially depending on the type of service.
A combination of health system–, provider- and patient-level variables affect the use of health services in Canada. More research is needed to determine why Black patients have higher mortality from certain cancers in Canada, and the reasons for infrequent access to cancer treatments in the US and UK cannot necessarily be extrapolated to the Canadian context. Routine collection of race and ethnicity data in registries could facilitate identification of key system and patient variables that affect access to cancer treatments. Learning how access to cancer treatments differs for Black patients compared with other populations in Canada could prompt further analysis of reasons for disparities, if they exist. This information could guide epidemiologists, clinical trial developers and health care providers to design targeted interventions to help equalize access to cancer care.
Enhanced use of culturally sensitive cancer care
Providing individualized, culturally sensitive cancer care is an important step to improving access to cancer screening, diagnosis and treatment in Canada. In a racially and socioeconomically diverse Toronto community health centre, Nnorom and colleagues23 implemented an Afrocentric education program on cancer screening and found that screening rates for breast, colorectal and cervical cancer increased from 17% to 72%, 18% to 67% and 59% to 70%, respectively, between 2011 and 2018. These data signify the impact that thoughtful, culturally sensitive interventions can have on access for vulnerable populations. Improving access to a regular family physician and, for some patients, a female physician, can also be important steps toward providing culturally sensitive care and eliminating disparities. For Black patients who already have a cancer diagnosis, culturally sensitive practices such as using multilingual lay health educators and virtual consultations can help to communicate information more effectively and increase adherence to cancer treatments.
Health and cultural literacy as tools to improve access to cancer care
Health literacy refers to a person’s ability to seek, process and comprehend medical information to make informed choices.24 Health literacy can also refer to the competencies and skills required to continue ongoing dialogue with family, community members and health care providers, which will ultimately shape health behaviours. An important domain of health literacy is cultural literacy, and this describes how a person’s social identity, beliefs and customs affect their medical decision-making. High levels of health literacy can help individuals discern the quality of the health information received, and communicate effectively with health care providers. The importance of the sociodemographic determinants of health literacy was highlighted in a study by Cudjoe and colleagues25 of African immigrant women undergoing cervical cancer screening. In this study, more than 75% of participants were proficient in English and more than two-thirds were college educated. This highly educated population had high levels of health literacy, which was associated with positive uptake of cervical cancer screening.
The Black population is heterogeneous in Canada, and can vary from first-generation Black African patients to second- and third-generation patients of African or Caribbean descent. These distinct patient populations have diverse cultural views and health understandings. Knowledge of the importance of health literacy highlights a need for health care providers to tap into cultural literacy in their Black patients (Figure 1). Framing health information in the context of a person’s cultural understandings of science and health requires the health care provider to have an awareness of the community that they serve. In a pilot study, use of culturally targeted videos were effective at increasing enrolment of Black patients in cancer clinical trials.26 These videos consisted of unscripted narratives of other Black patients describing their experiences with clinical trials, followed by physicians addressing any myths and reviewing facts in lay language. An Afrocentric lay health educator program in Toronto that improved breast and cervical cancer screening rates among Black patients also incorporated video testimonials featuring Black women.27 The lay health educators in this study were trained by Black women, further highlighting the importance of health care providers being representative of the population they serve.
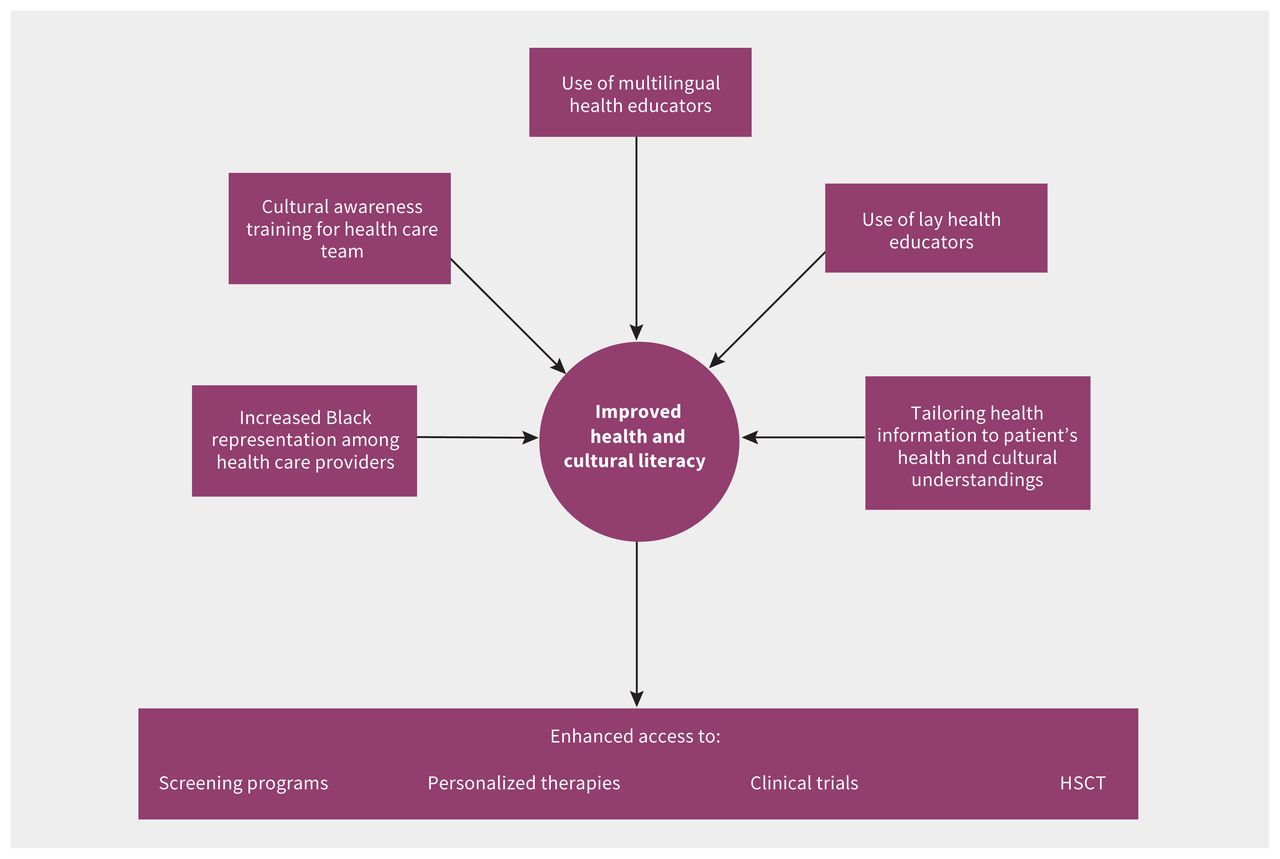
Improving access to cancer care in Black patients. Note: HSCT = hematopoietic stem cell transplantation.
Conclusion
Access inequities can threaten the Black community’s uptake of scientific advances in cancer care. Successful health care interventions have used culturally sensitive approaches to improve access to cancer care. Important measures that the medical community can embrace include improving representation of Black people in the health care team, using cultural awareness training for health care providers, using multilingual and lay health educators, and tailoring health information to a patient’s health literacy and cultural understandings. At the system level, Canadian race and ethnicity data are needed to fully understand where disparities remain and how thoughtfully designed interventions can improve access and outcomes in cancer care. Implementing evidence-based strategies will position the health care team to best meet the needs of a diverse population, while bridging gaps in equity. Research questions that need answering are listed in Box 1.
Box 1: Unanswered questions
How does access to unfunded tests and treatments differ among Black patients with cancer compared with non-Black patients? If differences are detected, what are the reasons behind these differences?
How do health and cultural literacy interventions affect uptake of novel cancer therapies?
How can we better predict which sources and types of media Black patients trust to receive their health information?
Footnotes
Competing interests: Doreen Ezeife reports receiving honoraria and travel support from Pfizer. She has participated on advisory boards with Pfizer, Bristol-Myers Squibb, Novartis and AstraZeneca. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Doreen Ezeife and Tony Truong conceived and designed the article. All of the authors contributed to data collection, analysis and interpretation. All of the authors drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

