


A 28-year-old woman presented to the emergency department with a 10-day history of vision loss. The patient was alert and oriented to place and time. She lived with her parents, who reported that she had not been eating much food for the past 3 months. She was socially isolated, reported a chronically depressed mood, and she drank about 1 L of distilled spirits daily. She had no history of drug use.
On physical examination, we found restricted abduction in both of the patient’s eyes, along with upbeat, gaze-evoked horizontal nystagmus (a video [Appendix 1] is available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.190998/-/DC1) and bradylalia. Her eye examination was notable for edema in the optic discs. Her pupils were mydriatic and isocoric, and the pupillary light reflex was attenuated in both eyes. She could not stand, and her limb muscles moved against gravity over the full range of motion. Fluid-attenuated inversion recovery magnetic resonance imaging (MRI) showed hyperintense signals in the bilateral medial thalami (Figure 1A) and in the periaqueductal grey matter (Figure 1B). We diagnosed Wernicke encephalopathy and started immediate intravenous thiamine replacement therapy. Her neurologic symptoms improved, and she was connected with mental health resources, including long-term medical social work. With the support of her family, our patient has abstained from drinking alcohol for 10 months.

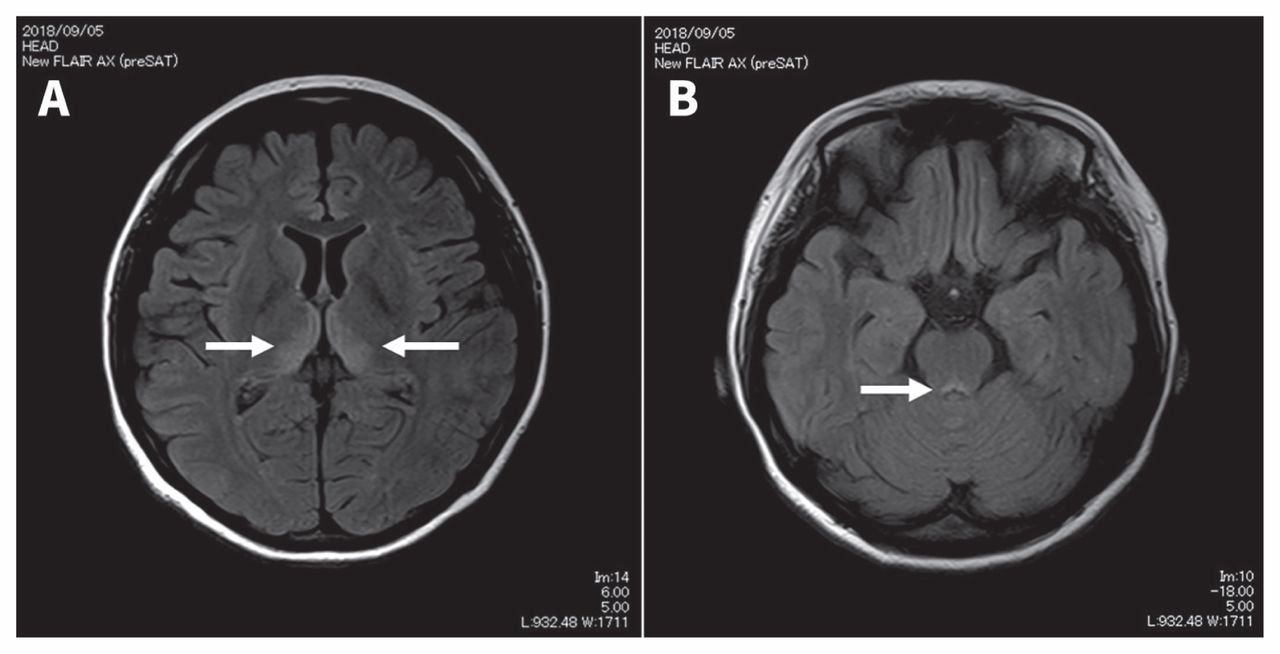
Fluid-attenuated inversion recovery magnetic resonance images of the brain of a 28-yearold woman with Wernicke encephalopathy showing hyperintense signals in the (A) bilateral medial thalami (arrows) and (B) in the periaqueductal grey matter (arrow).
Wernicke encephalopathy is a well-known complication of thiamine deficiency, mostly associated with alcohol use disorder.1,2 Classically, the syndrome comprises changes in mental status, gait ataxia and ophthalmoplegia.1,2 However, the full triad has been described in only 10% of cases.1 Patients with Wernicke encephalopathy usually do not present with disc edema, and we presumed our patient’s disc edema was caused by optic neuropathy unrelated to Wernicke encephalopathy.3,4 Left untreated, about 80% of patients with Wernicke encephalopathy acquire Korsakoff syndrome, which is characterized by memory impairment associated with confabulation.1,2 Common findings in MRI of the brain for Wernicke encephalopathy are hyperintense signals in the dorsal medial thalamic nuclei, periaqueductal grey area and the third or fourth ventricles.1,2,5
A video of upbeat, gaze-evoked nystagmus in a 28-yearold woman with Wernicke encephalopathy is available in Appendix 1, at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.190998/-/DC1
Acknowledgement
The authors thank Dr. Osamu Hasegawa, Department of General Medicine, Yokohama City University Medical Center, for useful discussions.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
Article extras
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

