


A well-appearing, 10-day-old, afebrile male presented to a pediatric emergency department with 24 hours of asymmetric arm movement without a history of trauma. The infant was large for gestational age (> 90th percentile), and he was born at term by spontaneous vaginal delivery. Maternal serologies, including syphilis, were negative. Maternal group B Streptococcus colonization was treated during labour.
In the emergency department, the infant had decreased spontaneous movement in his right arm and appeared to have a clavicular fracture on radiography (Figure 1A). He underwent an assessment for child maltreatment, including a skeletal survey, and the fracture was assumed to likely be related to birth. The infant was brought back for reassessment 10 days after the initial presentation, because the final radiography report did not document a clavicular fracture. Examination showed a well infant with a painful, internally rotated shoulder, extended elbow, flexed wrist, limp arm, weak grasp and asymmetric Moro reflex. Laboratory investigations showed thrombocytosis (465 [normal 150–400] × 109/L) and an elevated C-reactive protein level (65.6 [normal < 10.0] mg/L), with a normal leukocyte count. Findings on magnetic resonance imaging were suggestive of right proximal humerus osteomyelitis and glenohumeral septic arthritis (Figure 1B). Cultures of blood and synovial fluid samples grew pan-sensitive Staphylococcus aureus. Cefotaxime (50 mg/kg every 6 h) and joint débridement by orthopedic surgery led to marked improvement. After physiotherapy and 4 weeks of antibiotics, arm movement and power were normal.

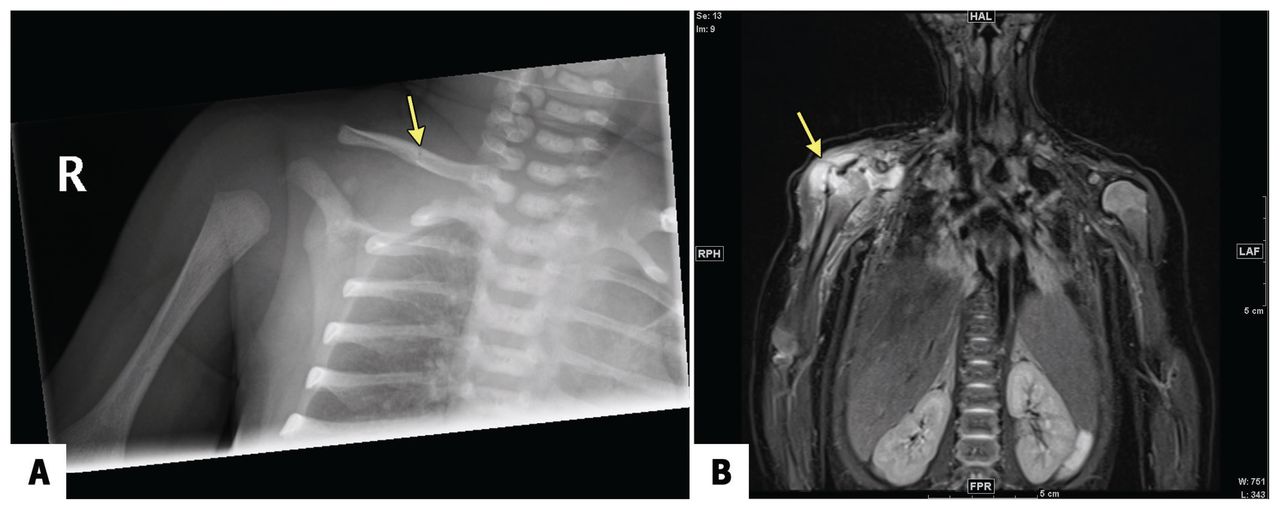
(A) Radiograph of a 10-day-old infant with asymmetric arm movement showing lucency in the midshaft of the right clavicle (arrow), initially interpreted to be a fracture, but subsequently thought to represent a nutrient vessel. (B) Magnetic resonance image showing osteomyelitis of the proximal epiphysis of the right humerus with a small intrachondral collection extending through the joint capsule into the adjacent anterolateral soft tissue. The large right glenohumeral joint effusion with diffuse synovial thickening and enhancement raised suspicion for associated septic arthritis. The image also shows diffuse edema of the surrounding soft tissues and muscles. The arrow denotes the affected arm. The areas of enhancement further highlight the affected tissues.
Neonatal joint and bone infections are rare (around 13/1 000 000 in pediatric studies)1 and are most commonly caused by S. aureus and β-hemolytic Streptococcus.1,2 Infants with joint and bone infections can present as afebrile and have normal bloodwork. The most common symptoms are pain, swelling and pseudoparalysis.2
Paralysis and pain are 2 major causes of decreased limb movement among neonates. Unilateral upper extremity paralysis is most often caused by brachial nerve palsy from birth-related brachial plexus injuries.3 Stroke is less common and typically presents with painless paralysis. Musculoskeletal pain may be caused by trauma, infection and space-occupying lesions. If traumatic injuries are found in a premobile infant, clinicians must consider inflicted trauma.
Treatment of neonatal joint and bone infections includes targeted antibiotics and surgical débridement, and most patients recover fully.2 Follow-up includes growth surveillance of the affected limb because of the risk of growth plate involvement, given its vascularity.
Clinical images are chosen because they are particularly intriguing, classic or dramatic. Submissions of clear, appropriately labelled high-resolution images must be accompanied by a figure caption. A brief explanation (300 words maximum) of the educational importance of the images with minimal references is required. The patient’s written consent for publication must be obtained before submission.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained parental consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article extras
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

