


A 46-year-old man presented to the emergency department having had 2 large, nonbloody vomits and abdominal pain over the preceding 3 hours. He had no history of gastresophageal reflux disease or other relevant medical conditions. He had a 20-year history of drinking 10–15 cans of beer a week. On examination, his abdomen was rigid and tender in the left upper quadrant. Laboratory results showed elevated leukocytes at 13.8 (normal 4.5–11.5) × 109/L with 77.8% neutrophils and high sensitivity C-reactive protein of < 0.02 (normal < 0.80) mg/dL. A chest radiograph showed pneumomediastinum (Figure 1A), and a subsequent computed tomography scan of the patient’s chest also showed pneumomediastinum and left hydropneumothorax (Figure 1B). We diagnosed Boerhaave syndrome, perforation of the esophagus.
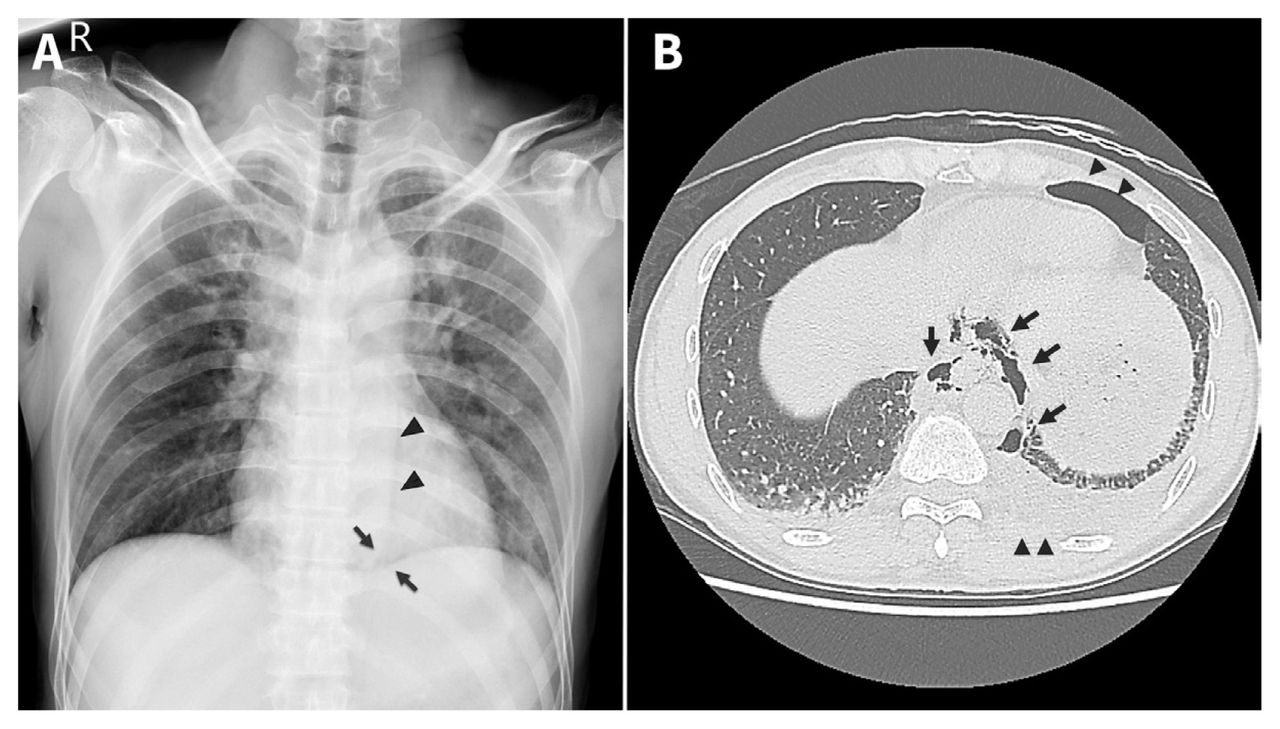
Boerhaave syndrome in a 46-year-old man. (A) Chest radiograph showing Naclerio’s V sign, which is the presence of air outlining the left, lower, lateral mediastinal border (arrows), with periaortic air streaks lateral to the descending aorta and above the left diaphragm (arrowheads). Naclerio’s V sign confirms pneumomediastinum. (B) Chest computed tomography scan showing pneumomediastinum (arrows) and left hydropneumothorax (arrowheads) suggestive of esophageal rupture.
The patient underwent esophageal repair and decortication of the pleura, with placement of a drainage gastrostomy and a feeding jejunostomy. During surgery, a 1.5 cm laceration was found at the lower thoracic esophagus (Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.202893/tab-related-content). Sixteen days after his operation, we stopped jejunostomy feeds when evaluation by esophagography showed no contrast leakage from the repair site. Two months later, he had made a full recovery.
Epidemiological data regarding esophageal perforation are sparse. A nationwide study in Iceland reported an annual incidence of 3.1 per million people.1 A careful history and examination may help determine the cause and site of perforation. A systematic review reported that the most common causes of oesophageal perforation are iatrogenic (46.5%), spontaneous (38%) and foreign body (6%).2 More than 70% of perforations are thoracic, such as with our patient, and typical symptoms include acute epigastric and substernal chest pain, shortness of breath and subcutaneous emphysema, after forceful vomiting.2–4
Boerhaave syndrome is a transmural perforation of the esophagus that differs from a Mallory–Weiss tear, which is a nonpenetrating mucosal laceration of the distal esophagus near the gastresophageal junction.5 Both are more common in men who consume excessive alcohol and are linked to barotrauma of the esophagus; however, hematemesis is common in Mallory–Weiss, but not Boerhaave, syndrome. 5 Treatment depends on the severity of the perforation, and case reports have described recovery after conservative, endoscopic and surgical intervention.3 The risk of death is about 13%.2
Footnotes
Competing interests: None declared.
The authors have obtained patient consent.
This article has been peer reviewed.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

