


Although medical education has historically excluded and devalued trainees with disabilities, inclusion of these students can be beneficial to health systems.
Technical standards and inflexible admission criteria exclude students with disabilities who would be capable of safe and effective practice, ignoring the strengths that living with disabilities can impart.
No publicly available data on the number of medical students or applicants with disabilities in Canada are available, perpetuating the status quo of discrimination through an absence of monitoring, transparency and accountability.
Effective accommodations policies must be consistent, transparent, considerate of intersectionality and informed by people with lived experience.
The 2023 recipient of the Canadian Medical Association’s Dr. Ashok Muzumdar Memorial Award for Physicians with Disabilities is Dr. Jessica Dunkley.1 One of the first Deaf physicians to practise in Canada, Dr. Dunkley won a landmark human rights tribunal case after she was denied accommodation for American Sign Language interpretation and dismissed from her residency program. Like Dr. Dunkley, many physicians with disabilities leverage their lived experience to act as champions for their patients, colleagues and trainees. In 2010, the Association of Faculties of Medicine of Canada (AFMC) released 10 evidence-based recommendations for undergraduate medical education in Canada,2 one of which emphasized that, in the spirit of their social accountability mandates, faculties must “recruit, select, and support” medical student classes that are “representative of the Canadian population.” The report noted that this involves addressing perceived and real barriers to the inclusion of underrepresented student groups and performing research to assess the impact of changes made to address these barriers. However, the Canadian medical school admissions process still presents barriers to applicants with disabilities, which are compounded by intersecting identities such as race, socioeconomic status and sexual identity.3 Although countries like the United States, Australia and New Zealand have developed national guidance on inclusion of applicants and students with disabilities,4,5 standardized guidance for Canadian admissions committees is absent beyond the legal duty to accommodate students with disabilities to the point of “undue hardship,” 6 leading to variation in the types of accommodations that may be available to such applicants. We discuss the barriers encountered by applicants to Canadian medical schools with disabilities and provide suggestions for remediation.
Do physicians with disabilities benefit patients and the health care system?
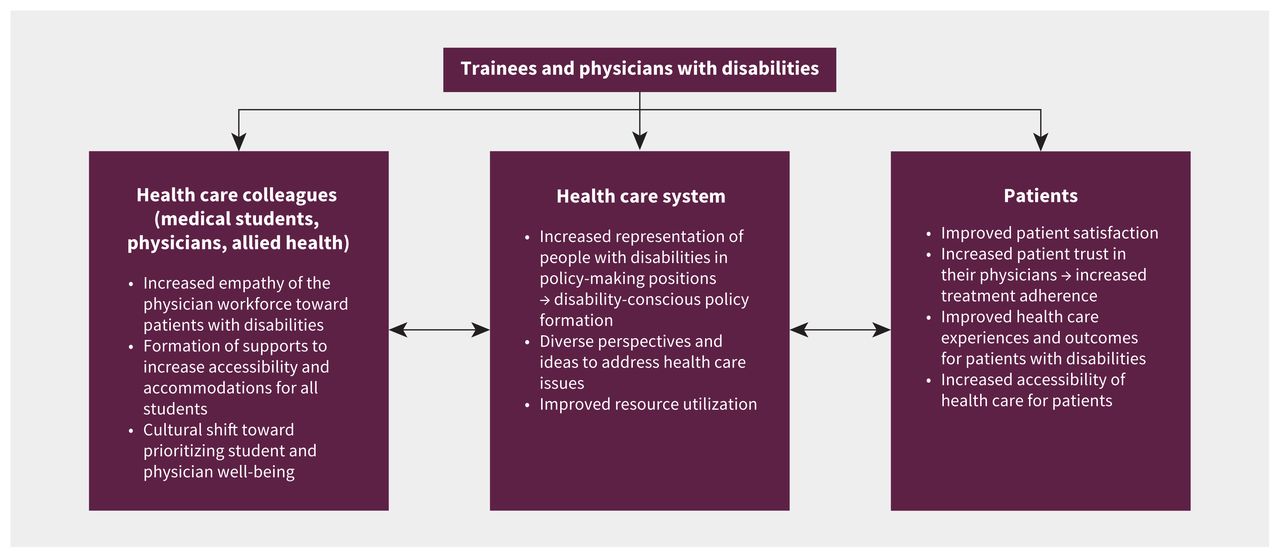
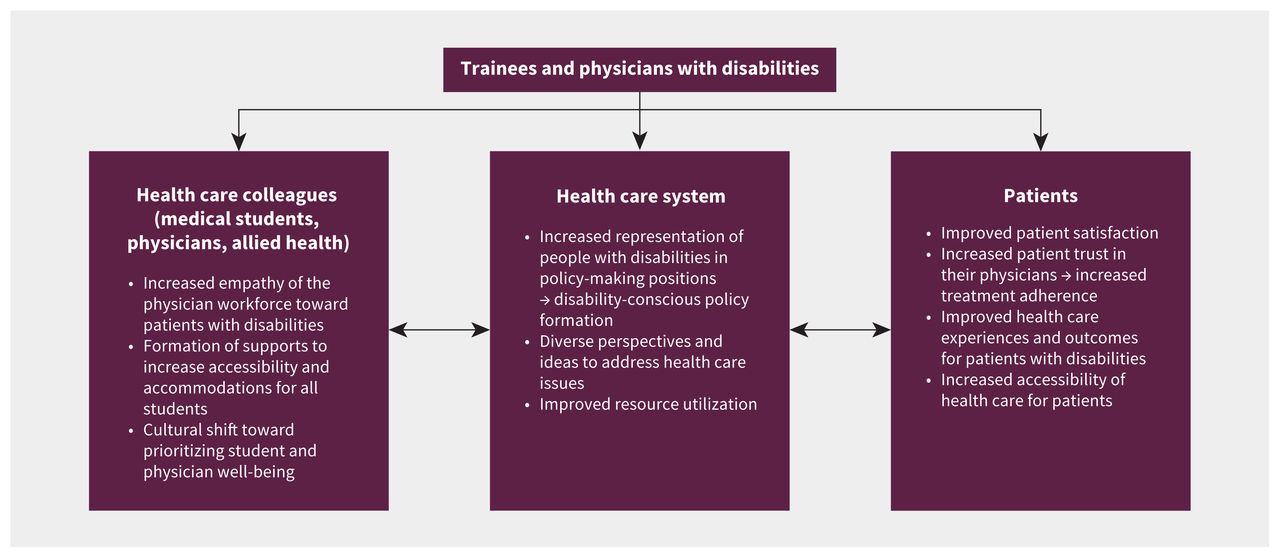
Disability is a diverse concept defined by the Accessible Canada Act as “any impairment […] that, in interaction with a barrier, hinders a person’s full and equal participation in society,”7 and is not inherently a deficit. Many physicians with disabilities have unique strengths and abilities to empathize with patients, which may lead to improved patient satisfaction, health care resource utilization and even patient outcomes (Figure 1).4,8–11 Engagement of physicians with disabilities in decision-making regarding health resource distribution and policy may also improve justice and equity for patients with disabilities.10,11
What medical school admissions processes disadvantage students with disabilities?
Stereotyping and ableist culture
Ableism has long been entrenched in the culture of medicine,11 driven by an illusion of a binary between sick and well that is perpetuated by societal, social and psychological influences.12 A commonly reported concern regarding admitting students with disabilities is the assumption that they will not be able to withstand the rigours of medical training or be able to undertake a broad scope of practice upon graduation. This argument does not consider the heterogeneity of disability nor the utility of and options for accommodation in training and practice. Stereotyping may occur when assumptions about limitations of a disability are made without a complete understanding of the student’s scope of abilities.3 Applicants to American medical schools have described being instructed by admissions officers to hide their disabilities during interviews to minimize the risk of bias, and report being asked inappropriate questions about their personal health when they cannot.11 Indeed, trainees with disabilities frequently take steps to hide their disabilities to avoid prejudice, perpetuating the illusion that they do not exist.
Inflexible admission criteria and technical standards
We reviewed publicly available, accessibility-related admission policies for the 2022–2023 admission cycle at all English-speaking Canadian medical schools.13 Exclusionary eligibility criteria that may disproportionately affect students with disabilities are summarized in Table 1.
Eligibility criteria of English-speaking medical schools in Canada in the 2022–2023 admission cycle that may disproportionately affect applicants with disabilities13
Criteria used to evaluate applicants for admission to medical school typically include grade point average (GPA), extracurricular activities, standardized testing (e.g., Medical College Admission Test [MCAT], Computer-Based Assessment for Sampling Personal Characteristics [CASPer]) and requirements for full-time course loads for all or part of the applicant’s undergraduate degree.13 Certain disabilities may affect grades or test scores if the learning environment is not adequately accessible, making these measures poor predictors of future performance as a physician in a properly adapted workplace. Although some schools offer opportunities for applicants to explain circumstances that affected such elements of their applications,13,14 others state explicitly that “the Admissions Office will not make any exceptions to declared policies.”15 This inflexible approach preferentially selects for applicants unaffected by illness or disability. However, the merits of a student who persevered through their undergraduate degree with serious illness are not captured in restrictive forms if, for instance, that student was unable to participate in many extracurricular activities,14 and the student may be outright disqualified if they studied on a part-time basis.15
Canada’s medical schools also require applicants to confirm that they meet technical standards to ensure that matriculants will be capable of medical practice once they graduate.16 These documents include statements that students with disabilities are “entitled to reasonable accommodation;”17 however, certain standards may not be met by applicants with some disabilities despite accommodations. In these cases, it may be possible to find alternatives that ensure the competence of the future practitioner. For example, for the technical skill of observation, students in Ontario must be able to “acquire all relevant sensory information,” such as auscultating heart sounds.17 Yet, Deaf physicians have been successfully trained in Canada with access to interpreters.1 Students must “execute motor movements reasonably required to provide general and emergency medical care,”17 raising the question as to whether it is enough to be able to direct cardiopulmonary resuscitation or whether the individual must physically be capable of performing it independently.11 Medical school has long been structured around the notion that to be any type of physician, you must be capable of being every type of physician. 12 In this way, generic technical standards deny students entry into fields in which they may excel.
Admission policies directly addressing accessibility vary considerably among medical schools. Several notable policies are highlighted in Table 2 and Table 3. The Ontario Medical School Application Service (OMSAS) has recently introduced a space for disability-based consideration requests in the application to Ontario medical schools.14 However, several aspects of this policy may limit its effectiveness in facilitating applications from applicants with disabilities. The consideration requests are available only to students who were unaccommodated during their undergraduate training, assuming that previously received accommodations sufficiently mitigated adverse effects of disabilities. The request applies only to the initial phase of file review, meaning that the consideration may not apply to full post-interview file review, potentially disadvantaging applicants with disabilities. The request requires an additional statement describing a plan to ensure success in the practice of medicine, putting the onus on the student to outline a plan without knowledge of available institutional resources. The request also requires provision of medical documentation, raising privacy challenges and risking further discrimination.
Features of the Ontario Medical School Application Service (OMSAS) disability-based consideration request system and associated concerns14
Lack of information regarding accommodations
We found no information on admissions websites about what types of accommodations may be possible during interviews or medical training for students to view without personal disclosure. Many students avoid disclosure for fear of stereotyping, discrimination and even outright exclusion.4,11 As with the OMSAS accommodation request, 1 school asks students to inform them of future accommodation needs for medical school before interviews, warning that matriculation is dependent on review by an accommodations committee.18 Given the time and cost involved in applying to medical school, this absence of information may discourage students from applying at all.5
What data are needed to inform accessible admission policies?
Data on disabilities among Canadian medical students are limited, albeit with some recent improvements.21 The AFMC added questions about physical limitations, learning disabilities and mental health concerns to their MD Entry Questionnaire in 2019 and Pre-clerkship Questionnaire in 2021; disability is currently not addressed in the AFMC Graduation Questionnaire.22 These data are not publicly available but can be accessed for research purposes with research ethics board approval. For the first time, in 2023, the Canadian Resident Matching Service released information on the combined percentage of Canadian and international residency applicants who self-identified as having a disability at 5.1%,23 a rate far lower than the 22% prevalence in the general Canadian population.24
Gathering comprehensive quantitative and qualitative disability-related data has had a positive impact in other countries. Up-to-date American data on the prevalence of medical students stratified by disability type, percentage of students seeking accommodations, barriers to help-seeking and clinical performance of medical students with disabilities have facilitated the formation of comprehensive guidelines on inclusive admissions and on how to support medical students once accepted.3 In particular, data characterizing types of disability help institutions understand the heterogeneity of disability and corresponding accommodation needs.21 Longitudinal data comparing disability prevalence among applicants, interviewees and accepted students is also essential to identify barriers and track progress.21
What can Canadian faculties of medicine do to support applicants with disabilities?
In light of the described barriers, we propose that Canadian medical schools revise their admission policies to ensure that they do not disqualify or disfavour students based on characteristics that are the result of a disability, such as part-time undergraduate course loads or reduced GPA during times of illness. Some schools address this on a case-by-case basis with options for students to explain circumstances that affected their studies but contributed to their personal growth in other ways (Table 1), although transparency is lacking regarding how these are evaluated. Medical schools should have publicly available resources for prospective applicants that detail the ways in which their programs are accessible to students with disabilities, including possible accommodations for interviews, preclerkship and clerkship. Medical schools must be proactive in meeting their legal obligation to accommodate students to the point of undue hardship at each stage of the application process. Accommodation queries and requests should be handled confidentially by specially trained individuals who are not involved in applicant evaluation. Furthermore, the wording of technical standards should be revised to clarify where alternatives that do not compromise patient safety may be considered if the skills cannot be performed as stated, even with accommodations.17 Some schools in the US do this by employing functional technical standards, which emphasize the skills required to be an effective physician without dictating the exact means by which this must be achieved.25 Overall, increased transparency will empower students with disabilities to apply to medical schools with confidence that they will receive the accommodations they need, promote standardization of accommodations between schools and increase institutional accountability.
The inclusion of more people with disabilities in medicine will help counter biases and stereotypes through the acknowledgement of such people’s strengths and abilities.3 Increased representation of allied health care workers and community members with disabilities as interview evaluators and on admissions committees should be rapidly implemented. In addition, anti-ableist training for admission committee members and interviewers may promote recognition of internalized biases and reduce discrimination.
Publicly available, comprehensive and up-to-date data on the prevalence and experiences of Canadian medical students with disabilities would enable identification and study of the effects of exclusionary policies so that steps can be taken toward increasing inclusion and equity.11 A comparative analysis should be performed and released regarding the prevalence of various disabilities among accepted and rejected applicants. Applicants who self-report data on disability status must do so freely and with informed consent. For privacy reasons, data must be deidentified, and any data that could be used to identify applicants must not be viewable to individuals who may influence student acceptance.
The creation of an AFMC-supported guideline for accessibility and inclusion for students with disabilities in Canada, parallel to those created by the Association of American Medical Colleges (AAMC) and the Medical Deans Australia and New Zealand,4,5 would set an evidence-based standard for schools to follow and to which they would be held accountable. Importantly, these institutions must consult students with lived experience when developing, implementing and evaluating disability-related policies and procedures to reduce the establishment of performative systems that appear to address gaps while failing to truly meet the needs of students with disabilities.
Most importantly, faculties must approach accessibility with creativity, openness and willingness to change. Virtual medical school interviews, for example, had never been permitted before the COVID-19 pandemic, even in cases of medical illness, but now remain common after the cessation of travel restrictions, given better accessibility. Large-scale changes can be implemented if accessibility is made a priority.
Conclusion
Despite evidence that patients, health care workers and society benefit from the inclusion of physicians with disabilities, admission policies for Canadian medical schools systematically exclude these individuals from the medical field. Accessible admission processes are an important step to increasing disability representation and eradicating ableism in medical culture.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Shira Gertsman conceived the work, and Shira Gertsman, Yasmin Dini and Devon Wilton contributed to its design, as well as data acquisition. All of the authors contributed to data analysis and interpretation. Shira Gertsman, Yasmin Dini and Devon Wilton drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

Article tools






{kind=link}
Jump to section
- Article
- Do physicians with disabilities benefit patients and the health care system?
- What medical school admissions processes disadvantage students with disabilities?
- What data are needed to inform accessible admission policies?
- What can Canadian faculties of medicine do to support applicants with disabilities?
- Conclusion
- Footnotes
- References
- Figures & Tables
- Related Content
- Responses
- Metrics
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections


Podcast