


Virtual overdose monitoring services use digital technologies, such as smartphone applications or phone lines, to provide a variety of supports focused on harm reduction, such as overdose monitoring, harm reduction education, and referrals to health and social services.
They can facilitate timely and anonymous access to emergency care for people who use substances.
During the first 14 months of operations, the National Overdose Response System monitored 2172 substance use events; 53 adverse events required emergency response and no fatalities were reported.
Based on emerging evidence, physicians may consider suggesting virtual overdose monitoring services as an additional option for harm reduction for people who are actively using substances and may require timely emergency support.
Further high-quality studies of promising virtual monitoring interventions that may improve outcomes for people who use substances are needed.
In 2021, 21 people in Canada died each day from poisonings associated with unregulated substance use.1 Despite several initiatives to combat the overdose crisis, overdose fatalities continue to rise, particularly since the start of the COVID-19 pandemic. Experts have suggested several policy initiatives, including decriminalization of drugs, safer supply of substances and expansion of supervised consumption services,2 but geographic, political and financial barriers have precluded the timely expansion of harm reduction services needed to reduce overdose-related deaths. We discuss the best available evidence regarding virtual overdose monitoring services as an additional option for enhancing timely access to harm reduction and overdose response, and describe our initial experience with such a service in Canada.
What are virtual overdose monitoring services and how are they delivered?
Isolation and solitary substance use, where people are unable to seek help, are the main drivers of overdose fatalities. We define virtual overdose monitoring services as those that use digital technologies, such as smartphone applications or phone lines, to provide a variety of supports focused on harm reduction, such as overdose monitoring, harm reduction education, and referrals to health and social services. Given the novelty of virtual overdose monitoring services, no consensus on their naming and scope of practice currently exists.
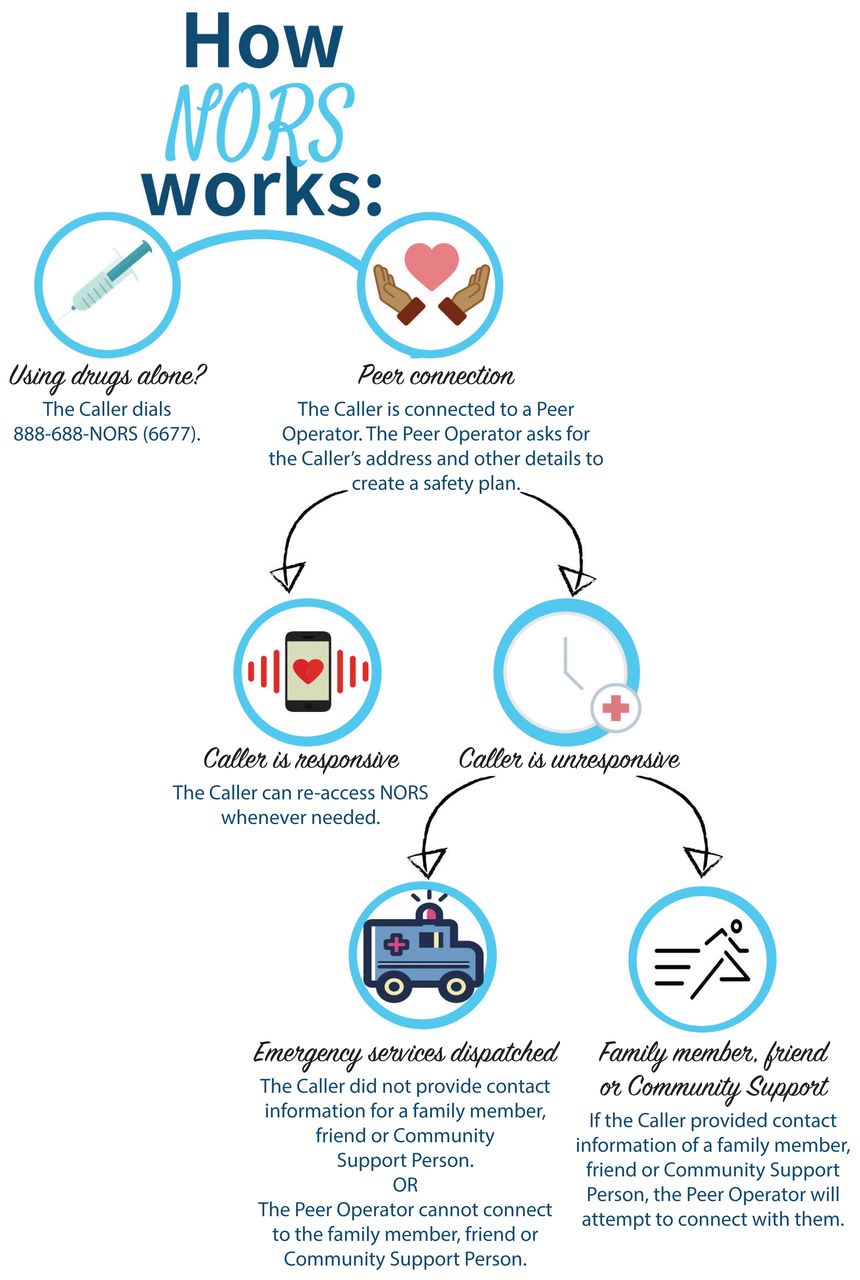
An example of a virtual overdose monitoring service is the National Overdose Response Service, a Canada-wide, toll-free phone line led and operated by people with lived, living or shared experience around drug use (Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220579/tab-related-content). At initial intake, callers connect anonymously with a peer operator to develop a personally tailored emergency response plan that can be activated during a suspected adverse event (e.g., overdose or drug poisoning, mental health crisis). Safer methods of use, such as use of smaller doses, are typically encouraged, along with referrals to health and social services. On subsequent calls, an overdose prevention operator monitors the caller throughout the duration of their episode of substance use. If an adverse event is suspected (e.g., lack of response, sounds indicating respiratory compromise), the operator activates the predetermined emergency response plan. Plans may include emergency medical services (EMS) via 911 dispatch or a prearranged individual contact capable of providing timely emergency care (e.g., cardiopulmonary resuscitation, naloxone administration). Figure 1 shows the operational flowchart for the National Overdose Response Service.

National Overdose Response Service (NORS) operational flowchart. Reproduced with permission from NORS.
Who is eligible to use virtual overdose monitoring services?
Virtual overdose monitoring services operate 24 hours a day using a variety of telecommunication platforms and are available to a diverse population of people who use substances. Services have no restrictions on substance type or route of administration — a unique feature given that most in-person supervised consumption services are not able to permit inhalation or smoking of substances owing to fire code regulations. In addition to the National Overdose Response Service, the Brave application provides virtual overdose monitoring services across Canada, as well as in the United States and the United Kingdom. The 3 other Canadian applications are the Connect smartphone application by LifeGuard (available in British Columbia and regions of Ontario), the Better App by Last Door (available in BC) and the Digital Overdose Response Service (available in Alberta). We are aware of 4 virtual overdose monitoring services in the US, namely the UnityPhilly (tested in Philadelphia, Pennsylvania, but currently offline), Naxos OD (active in South Bend, Indiana), and Canary applications, and the Never Use Alone hotline (Appendix 1).
What is the evidence of benefit of virtual overdose monitoring services?
Systematic reviews have shown that in-person, supervised consumption services prevent opioid-related deaths during acute substance use3 and mitigate the risk of secondary substance-related harms such as HIV transmission,4 particularly among people who inject substances.5,6 However, much less evidence is available for virtual overdose monitoring services. We found 7 studies that evaluated virtual approaches to harm reduction for people who use substances (Table 1), including 2 reviews and 5 primary studies of interventions that aligned with our definition of virtual harm reduction. Although the reviews showed promise and feasibility of virtual monitoring, most studies were undertaken in the context of the medical treatment for substance use disorders, whereas virtual overdose monitoring services tend to provide care focused only on harm reduction and facilitate access to timely emergency medical services.7,8 One primary study, conducted in BC, found that 68% of individuals who used substances and had a cellphone stated that they were willing to use technology-based solutions to mitigate the risks of overdose.11 A prospective study involving both people who used opioids and community members showed that laypeople were able to respond to 71 (95.9%) of 74 overdoses using technology, suggesting that equipping laypeople with naloxone and an emergency response application may successfully reverse overdoses in the community.12 Similarly, a study showed that a smartphone-enabled device for overdose detection that was capable of alerting naloxone-equipped laypeople or EMS may be a feasible harm reduction tool.10 A qualitative study found potential benefits of “drug spotting,” which is a longstanding, informal community practice whereby a person who intends to use drugs asks a friend, family member or person with lived experience to monitor their drug use via text, phone or video call.10
Summary of literature on virtual overdose monitoring services
Pilot data from the National Overdose Response Service
Between Dec. 15, 2020, and Feb. 28, 2022, operators with the National Overdose Response Service monitored 2172 substance use calls (222 unique callers; mean 9.8 calls per client, standard deviation 44.0); 53 (2.4%) required emergency response activation, with 2 false alarms. Staff contacted all clients who required an emergency response after their events to verify outcomes. Most calls originated in Ontario (n = 1315, 60.5%), followed by Quebec (n = 506, 23.2%) and Alberta (n = 144, 6.6%). Most were from urban areas (n = 2047, 94.2%). Of the 2273 reported types of drugs used, opioids (n = 1721, 75.7%) were the most frequent, followed by cocaine (n = 203, 8.9%), methamphetamine (n = 168, 7.4%) and unknown or not reported (n = 164, 7.2%). Of the 2242 routes of administration recorded, intravenous use (n = 1160, 51.7%) was most frequent, followed by smoking or inhalation (n = 872, 38.9%), insufflation (n = 61, 2.7%) and unknown or not reported (n = 106, 4.7%).
What are possible harms and limitations of virtual overdose monitoring services?
Harms associated with use of virtual overdose monitoring services are possible, but relative risks of harm are not known. For instance, emergency response times facilitated by these services will be slower than for an adverse event occurring in a supervised consumption site, where medically trained staff can provide immediate care.4 However, the pilot data from the National Overdose Response Service recorded no deaths among the 53 calls that required emergency response activation, suggesting that timely EMS response may yet be useful.
Compared with supervised consumption services, the quality of care facilitated by virtual overdose monitoring services may be limited owing to communication or technological barriers.6 For instance, virtual services require individuals to have reliable access to telephones or smartphone technology, including cellular or wireless Internet service. Additional limitations include the possibility of false-alarm calls caused by dropped calls or depleted telephone batteries. In such cases, emergency response may be activated when not strictly needed. One study found that 89 (30.6%) of 291 calls to UnityPhilly were false alarms.12
What can we expect in the future?
Virtual overdose monitoring services are novel public health interventions capable of providing timely and accessible harm reduction and overdose prevention services for people who use substances. Evidence, including pilot data from the National Overdose Response Service, suggests that virtual overdose monitoring services have promise as an adjunct to supervised consumption services in the continuum of care for people who use substances. However, more high-quality research is needed to better understand the potential benefits, as well as the risks and limitations, of virtual overdose monitoring services. Physicians may consider suggesting virtual overdose monitoring services as an adjunctive option for harm reduction, particularly to individuals who are actively using substances while facing barriers to accessing supervised consumption services. To advance the field, we suggest the development of standardized definitions and data collection systems (including a core outcome set), without creating barriers for accessing care. Ongoing program evaluation and research funded by Health Canada and codesigned with people of lived experience aims to further develop an evidence base around virtual overdose monitoring services.
Acknowledgements
The authors thank Kim Ritchie and Rebecca Morris-Miller from the National Overdose Response Service and Gordon Casey from the Brave Technology Co-Op for their relentless support and assistance. The authors also thank Caitlin Stokvis for the infographic design and Heidy Rechnitzer for help with application testing.
Footnotes
Competing interests: George Matskiv is an unpaid member of the board of directors for the National Overdose Response Service (NORS). Tyler Marshall and Dylan Viste are employees with the University of Calgary and receive salary via Health Canada’s Substance Use and Addiction Program, which provides operational funding for NORS. Oona Krieg is a co-founder of NORS, and the chief operating officer for Brave Technology Co-Op. Monty Ghosh is a co-founder and advisor for NORS, receives funding from Health Canada’s Substance Use and Addiction Program, and is a board member with the Canadian Society of Addiction Medicine.
This article has been peer reviewed.
Contributors: George Matskiv and Tyler Marshall contributed equally to this work and share first authorship. All authors contributed to the conception and design of the work, drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: None of the authors received any funding or reimbursement for writing this article. The National Overdose Response Service and the evaluation of the program have been funded by Health Canada’s Substance Use and Addiction Program (SUAP), as well as in-kind support from the University of Calgary, and the University of Alberta. Additional funding was provided by Healthcare Excellence Canada and The Canadian Institute of Health Research.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article tools






Jump to section
- Article
- What are virtual overdose monitoring services and how are they delivered?
- Who is eligible to use virtual overdose monitoring services?
- What is the evidence of benefit of virtual overdose monitoring services?
- What are possible harms and limitations of virtual overdose monitoring services?
- What can we expect in the future?
- Acknowledgements
- Footnotes
- References
- Figures & Tables
- Related Content
- Responses
- Metrics
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

