


Life-threatening emergencies, such as cardiac arrest, that occur at camps may be under-reported.
Myocarditis can cause cardiac dysrhythmias in children and can present with sudden cardiac arrest
Outcomes for cardiac arrest at any age are improved through immediate provision of effective cardiopulmonary resuscitation (CPR), early defibrillation and rapid access to advanced cardiac life support.
Widespread CPR training, including for employees and older youth, and placement of automated external defibrillators in an accessible location can improve outcomes of pediatric out-of-hospital cardiac arrest in camps.
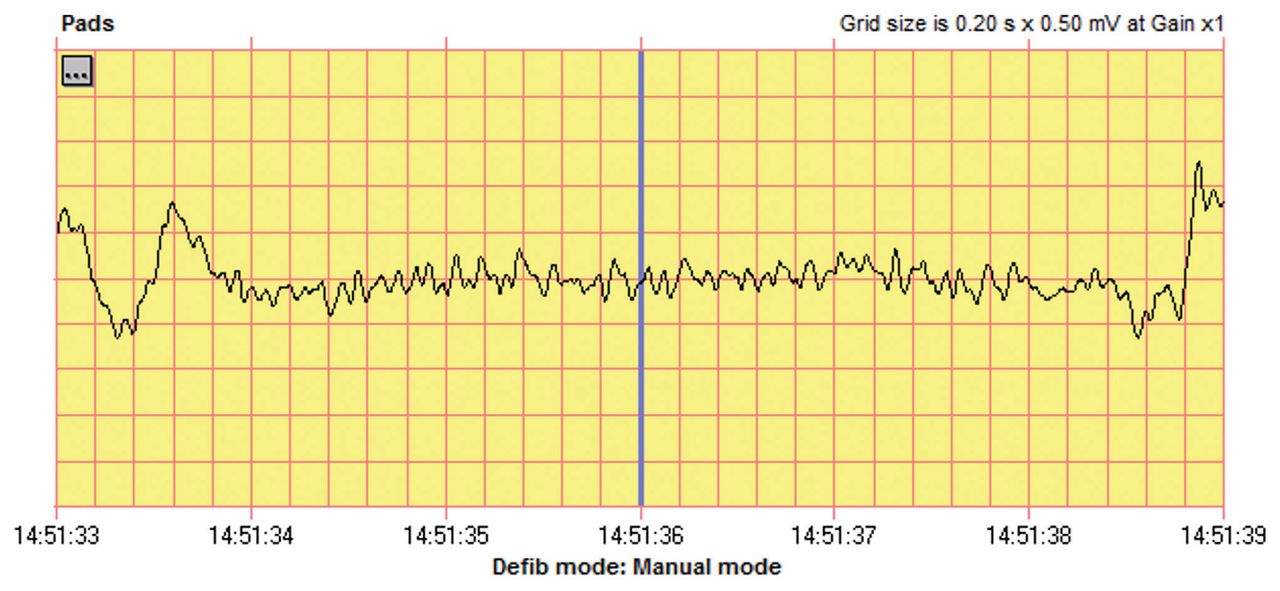
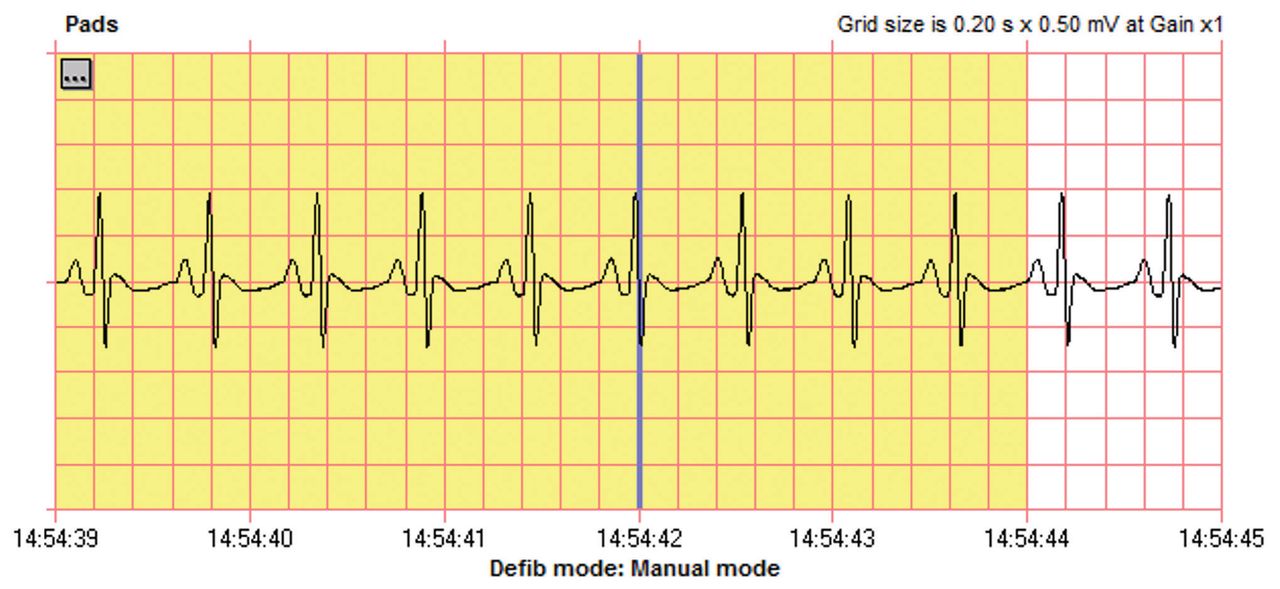
A previously healthy 14-year-old girl on no medications, with recent history of resolved coryza and cough, suddenly became unresponsive while sitting in her cabin at camp. A fellow camper did not feel a radial pulse and immediately initiated chest compressions while others called for help. Emergency medical services (EMS) were contacted and the camp’s health response team was activated by radio. The camp physician and 2 nurses arrived at the scene 4 minutes after cardiopulmonary resuscitation (CPR) was started. At that time, the patient had a palpable carotid pulse, absent brachial pulses and agonal respirations. The health professionals began artificial respiration (mouth-to-mouth) and restarted chest compressions 3 minutes later, after a rapid increase and then cessation in carotid pulse. An EMS team, consisting of primary care paramedics and firefighters, arrived 1 minute after chest compressions were restarted. The EMS team applied an automated external defibrillator (AED) 8 minutes after the onset of unresponsiveness. The AED detected ventricular fibrillation (Figure 1) and administered a standard 120 J shock, leading to ventricular tachycardia (Figure 2), followed by 15 seconds of narrow QRS waveform and then degeneration into ventricular fibrillation (Figure 3). Return of spontaneous circulation (ROSC) with narrow QRS waveform was ultimately achieved after an additional 2 minutes of chest compressions and delivery of a second defibrillation using 120 J (Figure 4). The total duration from unresponsiveness to ROSC was 10 minutes. Advanced care paramedics arrived 2 minutes after ROSC and secured the patient’s airway via endotracheal intubation, inserted a large-bore intravenous catheter, administered a bolus of saline and transported the patient to the local hospital. A glucometer reading taken in the advanced paramedic ambulance was 19.1 mmol/L. While updating the receiving hospital, crisis workers were dispatched to the camp to debrief and support the responders, campers and staff.

Electrocardiogram from an automated external defibrillator administered to a 14-year-old girl with cardiac arrest, showing ventricular fibrillation.

Electrocardiogram from an automated external defibrillator administered to a 14-year-old girl with cardiac arrest, showing ventricular tachycardia after the first defibrillation.

Electrocardiogram from an automated external defibrillator administered to a 14-year-old girl with cardiac arrest, showing return to ventricular fibrillation.

Electrocardiogram from an automated external defibrillator administered to a 14-year-old girl with cardiac arrest, showing return to normal sinus rhythm after chest compressions and 2 rounds of defibrillation.
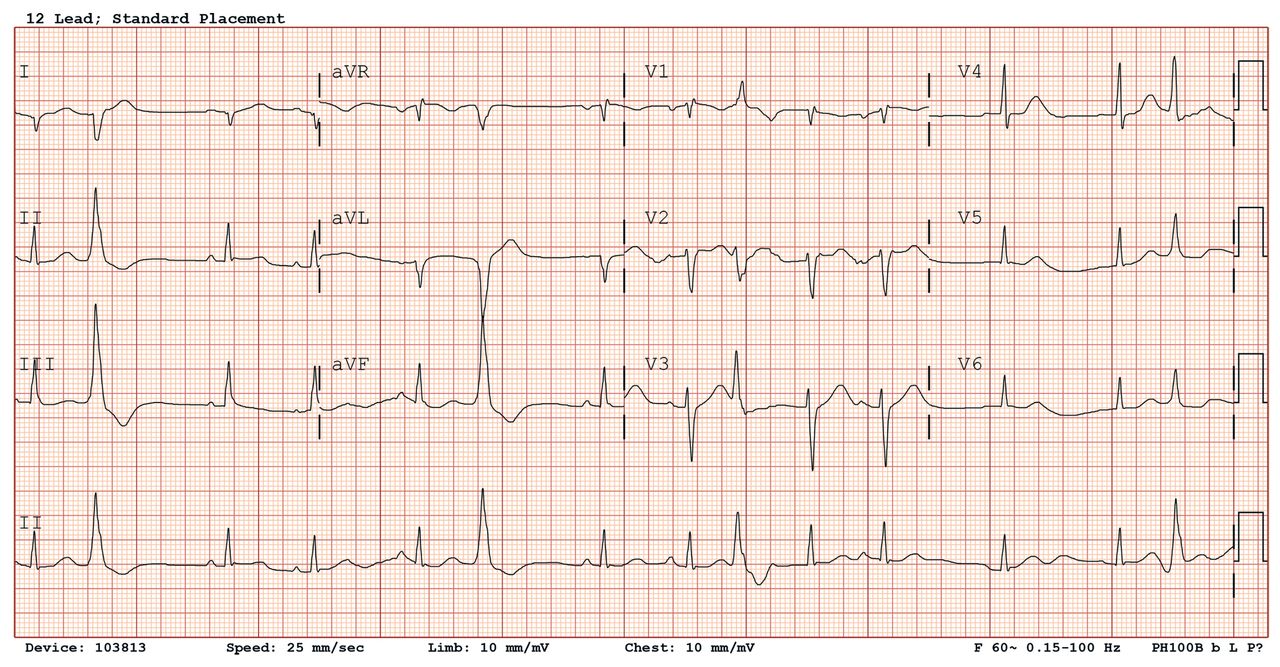
On arrival to the hospital emergency department, the patient’s temperature was 36.8°C, pulse 120 beats/min, blood pressure 105/80 mm Hg, respiratory rate 28 breaths/min, oxygen saturation 100% and end-tidal CO2 30 mm Hg. Her blood glucose was 11.7 mmol/L and subsequently normalized. Initial investigations showed a normal venous blood gas, complete blood count, and electrolytes; serum ketones were not detected. A urine toxicology screen was negative. A 12-lead electrocardiogram showed normal sinus rhythm with isolated right axis deviation but no evidence of hypertrophy or ST changes (Figure 5). A chest radiograph showed no cardiomegaly or consolidation, and good endotracheal tube position. A lidocaine infusion was started after a further brief episode of spontaneously resolving ventricular tachycardia was noted on the cardiac monitor.

Twelve-lead electrocardiogram of a 14-year-old girl with cardiac arrest, showing normal sinus rhythm with right axis deviation.
The patient was sedated and airlifted to a tertiary children’s hospital and admitted to the intensive care unit, where a diagnosis of myocarditis was confirmed by echocardiography and cardiac magnetic resonance imaging. The patient’s ejection fraction was 33%. In addition to supportive care, intravenous methylprednisolone (2 mg/kg/d) was administered. The patient was weaned off of sedation and extubated 48 hours after arrival. When asked about previous cardiac symptoms, she indicated that she had had intermittent palpitations on the morning of her arrest but no previous chest pain, shortness of breath or syncope.
The patient was discharged from hospital after 9 days on a weaning course of steroids. She had a normal neurologic examination with residual short-term memory loss. On follow-up 3 months after the arrest, her short-term memory loss had resolved and her ejection fraction was normal on repeat echocardiography.
Discussion
Overnight summer camps are common in Canada, though a specific census has never been done. Although injury and illness do occur at camp, medical emergencies are exceedingly uncommon across all age groups.1–4 Nevertheless, preparation for low-frequency, high-acuity emergencies are needed and should account for remote geography and prolonged EMS response times. Pediatric out-of-hospital cardiac arrest is uncommon but may be under-reported owing to inadequate surveillance systems, publication bias or legal concerns.
Survival after pediatric out-of-hospital cardiac arrest is 5%–10%,5,6 with survival among adolescents (estimated at 8.9%–15.8%) higher than among infants and younger children.7 Modifiable factors — such as early CPR, early AED use, early EMS attendance and quality of hospital care — can improve outcomes. 6–9 Unmodifiable factors include patient factors (e.g., age, comorbidity, cause of arrest) and features of the arrest (e.g., witnessed v. unwitnessed, initial rhythm).7 Widely available, public access to AEDs has allowed for earlier defibrillation, which is associated with higher rates of survival and better neurologic outcomes.10 Each additional minute of delay to shock is associated with an 8% decrease in 1-month survival.10 For our patient, a number of elements in her care contributed to her successful resuscitation and intact neurologic survival. She had a witnessed arrest by a fellow camper trained in basic life support, who immediately started CPR with good-quality compressions. The bystander was quickly supported by trained medical staff, employed by the camp. Fortunately, the camp was situated close to an EMS station; EMS personnel attended the scene quickly with immediate defibrillation, achieving ROSC within 10 minutes of initial unresponsiveness.
This case highlights the importance of early recognition and prompt initiation of effective compressions in the resuscitation of out-of-hospital cardiac arrest, regardless of age. Bystander CPR increases survival and improves neurologic outcomes by minimizing delays in establishing systemic blood flow.9 Bystander CPR can be supported in a camp by training all staff in basic CPR and maintaining skills through regular simulation.6,9 Response times can be further shortened by training willing older campers, support staff and other bystanders to perform compression-only CPR, which can be accomplished by watching a 60-second video.11 The societal benefits of widespread CPR training for youth and young adults are exemplified by this case, as the camper who recognized and started the resuscitation had received first aid training previously. Finally, this case offers a positive contrast to previous findings that bystander CPR occurs less frequently in pediatric out-of-hospital cardiac arrest, even when witnessed,6,9 underscoring the importance of training as many people as possible in CPR, with periodic practising of compressions.
Debriefing after an out-of-hospital cardiac arrest is important both for witnesses’ and providers’ psychological coping, and is vital for optimizing system performance.12 The campers present in the cabin during the time of the arrest underwent an immediate debrief by the camp physician and a camp director, with an appropriate crisis response to support their mental health. Crisis counsellors were made available for camp counsellors and others over the ensuing days. The camp health centre team and camp directors undertook a detailed analysis of system performance, which led to a number of changes. The AED is now stored in a portable bag containing other resuscitation equipment in a conspicuous location at the front of the health centre; this bag is assigned daily to 1 of the health centre staff, to be brought to a medical emergency declared on camp grounds. A second AED was purchased and placed near the cabins where the arrest occurred (a more remote area of the camp), secured against potential use for pranks. A camp policy, “Medical Emergency on Camp Grounds,” was developed to complement the existing health-related policies already in use, detailing roles in the event of an emergency, locations of AEDs and resuscitation equipment, and way-finding to assist EMS arriving at the camp.
Our patient had myocarditis, which is a common cause of out-of-hospital cardiac arrest and unexpected cardiac deaths in children.13 Myocarditis causes dysrhythmias due to cardiac inflammation, triggered primarily from a viral infection and associated cardiac dysfunction. Acute myocarditis has a biphasic presentation, with peaks in early infancy and mid-teenage years.14 Diagnosis can be clinically challenging as symptoms are wide-ranging and often nonspecific. Fulminant myocarditis is diagnosed when patients present with profound shock or acute arrhythmias, which can be fatal in the absence of advanced hemodynamic support.15 Treatment remains largely supportive, with ongoing debate over the benefits of anti-inflammatory therapies such as intravenous immunoglobulin or corticosteroids, and an overall 93% survival without transplant.15 Overall survival and long-term outcomes are highly dependent on both the severity and early recognition and treatment of this condition.
Footnotes
Competing interests: Alejandro Floh reports payment for expert testimony from the Office of the Chief Coroner of Ontario and participation on the safety monitoring board for clinical trials at the Hospital for Sick Children. Sheldon Cheskes reports funding from Zoll Medical, the Cardiac Arrythmia Network of Canada and the Heart and Stroke Foundation. He also reports honoraria for educational lectures on quality of cardiopulmonary resuscitation and participation on the advisory board of Drone Delivery Canada. No other competing interests were declared.
This article has been peer reviewed.
The authors have obtained patient consent.
Contributors: All of the authors contributed to the conception and design of the work. Herbert Brill drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

