


Abstract
Background: In Canada, only 15% of patients requiring palliative care receive such services in the year before death. We describe health care utilization patterns among home care users in their last 6 months of life to inform care planning for older people with varying mortality risks and evolving care needs as they decline.
Methods: Using population health administrative data from Ontario, we performed a retrospective cohort study involving home care clients aged 50 years and older who received at least 1 interRAI (Resident Assessment Instrument) Home Care assessment between April 2018 and September 2019. We report the proportion of clients who used acute care, long-term care, and palliative home care services within 6 months of their assessment, stratified by their predicted 6-month mortality risk using a prognostic tool called the Risk Evaluation for Support: Predictions for Elder-life in their Communities Tool (RESPECT) and vital status.
Results: The cohort included 247 377 adults, 11.9% of whom died within 6 months of an assessment. Among decedents, 50.6% of those with a RESPECT-estimated median survival of fewer than 3 months received at least 1 nonphysician palliative home care visit before death. This proportion declined to 38.7% and 29.5% among decedents with an estimated median survival between 3 and 6 months and between 6 and 12 months, respectively.
Interpretation: Many older adults in Ontario do not receive any palliative home care before death. Prognostic tools such as RESPECT may improve recognition of reduced life expectancies and palliative care needs of individuals in their final years of life.
Palliative care is an essential component of a holistic, comprehensive, and patient-centred approach to care for all people with a life-limiting illness from the time of diagnosis with the disease. 1–5 Early initiation of palliative care has been associated with improved end-of-life outcomes, such as improved quality of life, reduced distress, and better symptom management.6,7 Yet, the provision of palliative care is commonly misunderstood as being only for patients who are actively dying and in their last days or weeks of life.2 In Canada, estimates indicate that only 15% of the population receive palliative care in the home in their last year of life, with most visits being initiated in the last month of life and taking place within acute care settings.8–10 However, estimates suggest that more than 80% of deaths could benefit from a palliative care approach.9,11 Accurate and early recognition of palliative care needs by the clinical care teams is therefore essential. However, estimating survival beyond a few weeks may be challenging for clinicians, even for palliative care specialists,12,13 and predictions have been shown to be less accurate with longer prognostication time frames.12,14,15
We sought to determine the potential role of mortality-risk estimates generated from the Risk Evaluation for Support: Predictions for Elder-life in their Communities Tool (RESPECT), a validated tool for predicting 6-month mortality risk, in informing palliative care needs. Specifically, we examined the types of care and support (including palliative home care, acute care, and other institutional care) provided to a cohort of community-dwelling older adults within 6 months of their interRAI (Resident Assessment Instrument) Home Care assessment, stratified by their RESPECT-estimated median survival and vital status. We hypothesized that if current clinical assessments were as accurate as RESPECT, one would expect to observe higher intensity of palliative support provided to individuals with high mortality risk than to those with a lower estimated mortality risk.
Methods
We conducted a retrospective cohort study examining health care use among community-dwelling older adults in Ontario, Canada. Ontario has a publicly funded health insurance program (the Ontario Health Insurance Program), which includes services provided in the home and community settings. The study population consisted of adults aged 50 years and older who were eligible for publicly funded home care and received at least 1 interRAI Home Care assessment between Apr. 1, 2018, and Sept. 30, 2019.
Data sources
Record-level interRAI Home Care data were linked to other provincial health administrative databases housed and analyzed at ICES. ICES is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. The following databases were used to capture service use: National Ambulatory Care Reporting System for emergency department visits, Discharge Abstract Database for hospital admissions, Home Care Database for palliative home care visits provided by non-physicians, Ontario Health Insurance Plan for palliative home care visits provided by physicians, and Continuing Care Reporting System for long-term care admissions. Death date was captured using the Registered Persons Database. We used service recipient code 95 in the Home Care Database as it indicates that a patient’s service care goal involved being at the end of life or that the patient was provided services under an end-of-life designation. Only services provided by nonphysician providers (e.g., registered nurses and nurse practitioners, personal support workers, allied health professionals, and care coordinators) are captured in the Home Care Database. See Appendix 1, eTable 1 (available at www.cmaj.ca/lookup/doi/10.1503/cmaj.221513/tab-related-content) for all databases used in this analysis.
Mortality-risk estimation
RESPECT was originally developed using data collected through the Resident Assessment Instrument for Home Care on 435 009 community-dwelling older adults in Ontario, Canada, between Jan. 1, 2007, and Dec. 31, 2012.16 The algorithm has good discrimination (c-statistic 0.753, 95% confidence interval [CI] 0.750–0.756) and is well calibrated (intercept of calibration plot of 0.0146). We recently re-estimated and validated the algorithm, using a bootstrap sample, in contemporary interRAI Home Care data between Apr. 1, 2018, and Sept. 30, 2019 (n = 247 377); a description of this validation is available elsewhere (unpublished data, 2023). The re-estimated algorithm has similar performance as the original model (c-statistic 0.76, 95% CI 0.75–0.77; intercept of calibration slope of 0.88).
Baseline characteristics used as predictors in the RESPECT algorithm included sex assigned at birth; age at the time of assessment; physical function (dependence in activities of daily living [ADLs] or instrumental ADLs, and worsening ADLs); cognitive impairment (worsening decision-making capacity); diseases (stroke, congestive heart failure, coronary artery disease, Alzheimer disease and other dementias, multiple sclerosis, Parkinson disease, cancer, chronic obstructive pulmonary disease); health care use (number of hospital admissions or emergency department visits in the last 90 days); symptoms of reduced health (vomiting, edema, dyspnea, low fluid intake, weight loss, decrease in food or fluid consumption); prescription and receipt of life-sustaining therapies or treatments (chemotherapy, dialysis, oxygen therapy, ventilator or respirator); clinician diagnosis of an end-stage disease; and year of assessment and reason for assessment.
RESPECT groups home care clients with similar prognoses into 61 risk bins (Appendix 1, eMethods 1). The risk bins are based on the median survival derived from Kaplan–Meier survival curves and informed by recommendations of clinical experts who identified meaningful differences in life expectancies that would be helpful in decision-making. We extended the follow-up period to the most recent data available at the time of this study (i.e., June 29, 2022) to increase data completion for the Kaplan–Meier survival estimates. As the bin number increases, the 6-month mortality risk decreases and median survival increases. Between bins, the incremental increase in median survival can vary. For example, the incremental increase in median survival for bins 1–5 (i.e., individuals with high mortality risks) is less than 2 weeks, while increases in median survival for bins 56–61 (i.e., individuals with lower mortality risk) is nearly 2 months.
Outcomes
We followed home care clients prospectively to evaluate their health care use within 6 months following an interRAI Home Care assessment. The maximum follow-up was Mar. 30, 2020. Health care services included receipt of any acute care (hospital admission or emergency department visit), long-term care, or palliative care. Palliative care included palliative care home visits provided by nonphysician providers, such as registered nurses, palliative care home visits provided by physicians, and palliative care provided in hospitals. We calculated the proportion of home care clients who had at least 1 health care service day in the 6 months following an interRAI Home Care assessment. We also captured the intensity of health care use for each service, defined as the number of days in the hospital, emergency department (i.e., 1 day means a day with at least 1 emergency department visit), or long-term care home, and the number of palliative home care visits within 6 months of assessment. Palliative care provided in inpatient hospital settings was categorized based on the level of palliative care involvement as either high, medium or low based on the primary reason for admission, as well as the primary provider and involvement of palliative care specialist.17 Among home care clients who died within 6 months of assessment, we also reported the location of death (classified as acute care hospital, other institution, long-term care home, or community).
Statistical analysis
For this analysis, we collapsed the 61 RESPECT risk bins into 7 mortality-risk profiles. Each profile represents a survival range that marks a major stage of decline toward the end of life and reflects the current understanding of end-of-life trajectories across major causes of death.18 The first 3 mortality-risk profiles were defined based on predicted median survival as follows: assessments with a predicted median survival of less than 3 months (i.e., patients likely at the end of life), assessments with a predicted median survival between 3 and 6 months (i.e., patients likely approaching the end of life), and assessments with a predicted median survival between 6 and 12 months (i.e., patients likely in their last year of life). The remaining 4 mortality-risk profiles were defined based on predicted 6-month mortality risk as follows: between 20% and 33% (i.e., individuals who are likely not in their last year of life but have moderate–high mortality risk), between 10% and 20% (i.e., moderate–low mortality risk), between 5% and 10% (i.e., low mortality risk), and less than 5% (i.e., very low mortality risk).
The unit of analysis was the individual home care client. Long-stay home care clients are typically reassessed using the interRAI Home Care assessment every 6 months unless a change in health status requires more frequent assessment. Clients may therefore have multiple interRAI assessments within our study time frame. As such, 1 assessment was selected for each home care client at random.
Descriptive statistics were used to characterize service use, service intensity, and place of death for all home care clients according to their mortality-risk profile. Proportions, means with standard deviations (SDs), and medians with interquartile ranges (IQRs) were used to summarize continuous and categorical variables.
Two sets of analyses were conducted, first among a decedent cohort and second among the entire cohort (survivors and decedents). The decedent cohort included home care clients who died within 6 months following an interRAI assessment. Health care use includes any services received between the assessment date and death date among decedents, and between the assessment date and 180 days after the assessment date among survivors or decedents who died more than 6 months after the assessment.
Ethics approval
The use of data in this project is authorized under section 45 of Ontario’s Personal Health Information Protection Act and does not require approval by a research ethics board. Our approach adheres to the Strengthening the Reporting of Observational Studies in Epidemiology Statement: Guidelines for Reporting Observational Studies.19
Results
The cohort included 247 377 community-dwelling older adults with at least 1 interRAI Home Care assessment (Appendix 1, eFigure 1). Within 6 months of an assessment, 29 420 (11.9%) of clients had died (Table 1). Median survival and predicted 6-month mortality ranged from 30 days and 98.1% in RESPECT risk bin 1 to 1576 days (4.3 yr) and 1.6% in bin 61 (Appendix 1, eTable 2, eFigure 2).
Mortality-risk profiles: predicted 6-month mortality risk, sample size, and median survival
The mean age was 80.1 (SD 11.0) years at the time of assessment, and most clients were female (61.9%) (Table 2). Many comorbidities (congestive heart failure, coronary artery disease, cancer, and chronic obstructive pulmonary disease) and all symptoms of health instability, except vomiting, were more prevalent among higher-risk profiles (Table 3). Only a small proportion (2.6%) of home care clients had received a clinician diagnosis of an end-stage disease; this was more prevalent in the highest mortality-risk profile (77.9%). Most clients (74.5%) required extensive assistance (score of ≤ 4) in performing instrumental ADLs, and half (50.3%) reported worsening capacity to perform ADLs in the last 3 months, which was more prevalent among the highest mortality-risk profiles (96.1% v. 20.3%) (Table 4).
Baseline characteristics across the total cohort and stratified by mortality-risk profile
Health characteristics (diseases, symptoms, and health care service use) across total cohort and stratified by mortality-risk profile
Functional and cognitive status across total cohort and stratified by mortality-risk profile
Survival
The median survival was 58 (IQR 19–181) days among those with a predicted median survival of fewer than 3 months, 144 (IQR 47–466) days among those with a predicted median survival between 3 and 6 months, and 268 (IQR 79–826) days among those with a predicted median survival between 6 and 12 months (Table 1). Kaplan–Meier survival estimates for the 7 mortality-risk profiles are presented in Appendix 1, eFigure 3. The predicted 6-month mortality risk for the 3 highest-risk profiles was 86.8%, 63.2%, and 39.8%, respectively.
Within our cohort, 75.0% of individuals with a predicted median survival of fewer than 3 months, 55.4% of individuals with a predicted median survival between 3 and 6 months, and 40.7% of individuals with a predicted median survival between 6 and 12 months died within 6 months of an interRAI Home Care assessment (Table 1). Most deaths were attributable to terminal illness or organ failure, while 1.9% to 2.5% of individuals in the top 3 mortality-risk profiles experienced sudden death (Appendix 1, eTable 3).
Place and length of care
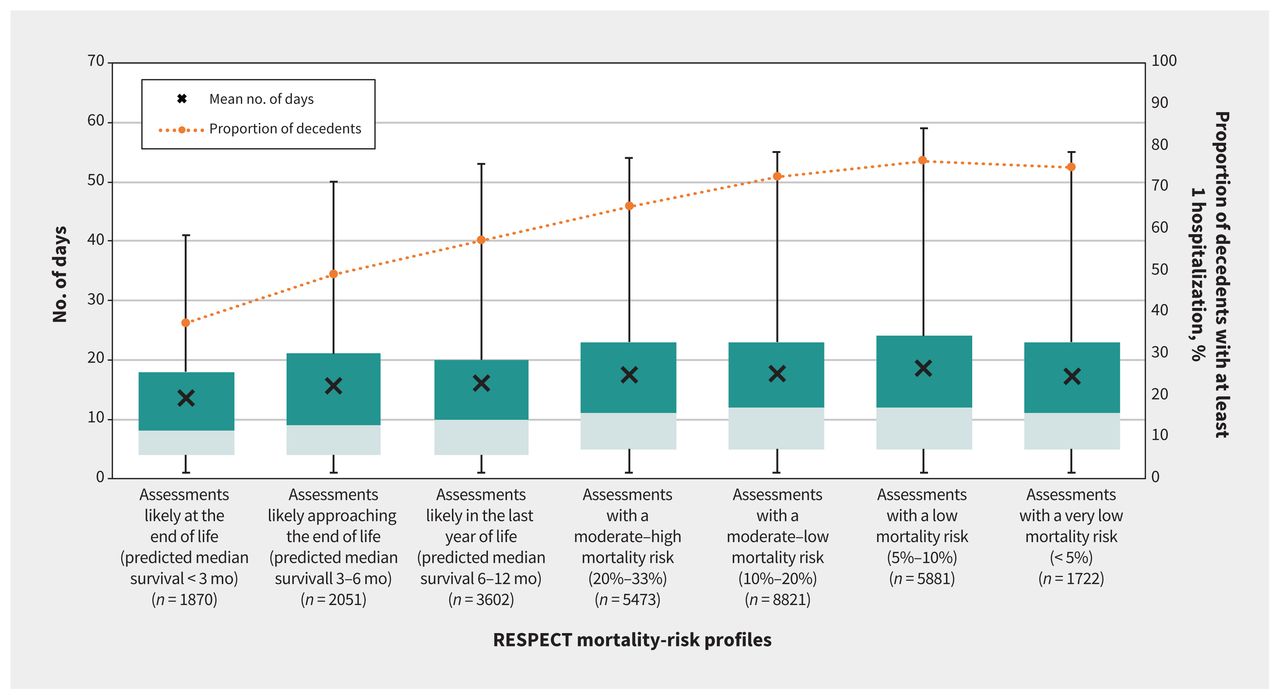
In the analysis of home care clients who died within 6 months after the interRAI assessment, among those with an estimated survival of fewer than 3 months, half (50.6%) received at least 1 palliative home care visit by a nonphysician (Figure 1 and Appendix 1, eTable 4) and less than a third (27.8%) received at least 1 palliative home care visit by a physician (Figure 2 and Appendix 1, eTable 4). The median number of nonphysician visits was 29 (IQR 10–71), and the median number of physician visits was 1 (IQR 1–3). The proportion of individuals who received at least 1 nonphysician palliative home care visit declined to 38.7% among those with a median survival between 3 and 6 months and to 29.5% among those with a median survival between 6 and 12 months. A sensitivity analysis excluding individuals who died suddenly produced similar results (Appendix 1, eTable 5). The median number of visits was 31 (IQR 13–71) among those with a median survival between 3 and 6 months and 27 (IQR 10–61) among those with a median survival between 6 and 12 months. The proportion of individuals who received at least 1 physician-provided palliative home care visit remained at 28.3% among those with a median survival between 3 and 6 months and 26.1% among those with a median survival between 6 and 12 months. The corresponding median number of visits was 1 (IQR 1–2) for both mortality-risk profiles.

Proportion of decedents with at least 1 palliative home care visit provided by a nonphysician and distribution of the number of visits within 6 months of an interRAI Home Care assessment, as illustrated by the box and whisker plots. The lower and upper boundaries of the boxes represent the first and third quartile values. The boundaries between the darker and lighter shaded areas represent the median value. The “whiskers” extending from the top and bottom of the boxes represent the 95% confidence intervals. Note: interRAI = Resident Assessment Instrument, RESPECT = Risk Evaluation for Support: Predictions for Elder-life in their Communities Tool.

Proportion of decedents with at least 1 palliative home care visit provided by a physician and distribution of the number of visits within 6 months of an interRAI Home Care assessment, as illustrated by the box and whisker plots. The lower and upper boundaries of the boxes represent the first and third quartile values. The boundaries between the darker and lighter shaded areas represent the median value. The “whiskers” extending from the top and bottom of the boxes represent the 95% confidence intervals. Note: interRAI = Resident Assessment Instrument, RESPECT = Risk Evaluation for Support: Predictions for Elder-life in their Communities Tool.
Individuals in the top 3 highest mortality-risk profiles who received at least 1 palliative home care visit (from either physicians or nonphysician home care providers) within 6 months of an assessment were comparable in clinical characteristics (e.g., symptom burden, pain, comorbidities, performance of instrumental ADLs, and worsening performance of ADLs) to those who did not receive palliative home care (Appendix 1, eTable 6). However, those who did not receive palliative home care were more likely to have not been identified by a clinician as being in their last 6 months of life, have higher levels of ADL dependency, experience worsening decision-making capacity, and have had at least 1 inpatient admission (Appendix 1, eTable 6).
Emergency department visits were the most frequently used type of institutional care across all risk profiles. The proportion of individuals with at least 1 emergency department visit in the 3 highest mortality-risk profiles were 41.3%, 55.2%, and 63.4%, respectively (Figure 3 and Appendix 1, eTable 4). The median number of days in the emergency department (i.e., the number of days with at least 1 emergency department visit) was 1 (IQR 1–2) across all 3 profiles. The corresponding proportion of individuals admitted to hospital at least once within 6 months was 37.4%, 49.2%, and 57.3%. The median number of days in hospital in the 3 highest mortality-risk profiles were 8 days (IQR 4–18), 9 days (IQR 4–21), and 10 days (IQR 4–20) (Figure 4 and Appendix 1, eTable 4). Most (57.8%, 59.6%, 57.9%) hospitalized individuals in the highest 3 risk profiles did not receive inpatient palliative care (Appendix 1, eFigure 4). Of those who received inpatient palliative care, the level of palliative care involvement was, in most cases, medium, with 10.1%, 7.2%, and 8.3% of those in the highest-risk profile receiving a high level of palliative care involvement. Among individuals in the 3 highest-risk profiles, 12.9%, 15.9%, and 16.3% were admitted to a long-term care home within 6 months (Figure 5 and Appendix 1, eTable 4).

Proportion of decedents having at least 1 day with an emergency department visit and distribution of the number of days within 6 months of an interRAI Home Care assessment where at least 1 emergency department visit had occurred. The distributions are illustrated by box and whisker plots. The lower and upper boundaries of the boxes represent the first and third quartile values. The boundaries between the darker and lighter shaded areas represent the median value. The “whiskers” extending from the top and bottom of the boxes represent the 95% confidence intervals. Note: ED = emergency department, interRAI = Resident Assessment Instrument, RESPECT = Risk Evaluation for Support: Predictions for Elder-life in their Communities Tool.

Proportion of decedents with at least 1 acute care hospital admission and distribution of hospital admission days within 6 months of an interRAI Home Care assessment, as illustrated by the box and whisker plots. The lower and upper boundaries of the boxes represent the first and third quartile values. The boundaries between the darker and lighter shaded areas represent the median value. The “whiskers” extending from the top and bottom of the boxes represent the 95% confidence intervals. Note: interRAI = Resident Assessment Instrument, RESPECT = Risk Evaluation for Support: Predictions for Elder-life in their Communities Tool.

Proportion of decedents admitted to a long-term care facility and distribution of days in long-term care within 6 months of an interRAI Home Care assessment, as illustrated by the box and whisker plots. The lower and upper boundaries of the boxes represent the first and third quartile values. The boundaries between the darker and lighter shaded areas represent the median value. The “whiskers” extending from the top and bottom of the boxes represent the 95% confidence intervals. Note: interRAI = Resident Assessment Instrument, LTC = long-term care, RESPECT = Risk Evaluation for Support: Predictions for Elder-life in their Communities Tool.
In the analysis of the entire cohort, including those who survived for more than 6 months after the interRAI assessment, the proportion of all individuals who received at least 1 nonphysician palliative home care visit was 46.1% among those with a median survival of fewer than 3 months, 30.5% among those with a median survival between 3 and 6 months, and 18.1% among those with a median survival between 6 and 12 months (Appendix 1, eFigure 5). The median number of nonphysician palliative home care visits received in these groups was 36 (IQR 12–98), 44 (IQR 16–113), and 38 (IQR 13–107), respectively. The corresponding proportion of all individuals who received at least 1 physician-provided palliative home care visit was 27.8%, 26.1%, and 23.3% with a median number of 1 (IQR 1–2), 1 (IQR 1–2), and 1 (IQR 1–3) visits, respectively. Trends of these outcomes across mortality-risk profile groups was similar to those in the analysis limited to decedents alone. However, unlike what was observed among decedents, the proportion of assessments with at least 1 day of institutional care follows an inverted U-shaped relation, which peaked in assessments with a median survival between 6 and 12 months.
Place of death
Nearly half (43.3%) of those with a prognosis of fewer than 3 months died in the community, and 9.9% died in a long-term care home (Appendix 1, eFigure 6). However, community-based deaths were comparably higher among individuals with a prognosis of fewer than 3 months than among those with a prognosis of 3 to 6 months (34.7%) and 6 to 12 months (30.1%).
Interpretation
In this study, we described health care utilization patterns among home care clients across mortality-risk profiles generated from RESPECT.16 We found that individuals who were identified as being likely at the end of life, based on a median survival of fewer than 3 months, were more likely to receive a nonphysician-provided palliative home care visit and less likely to receive institutional care provided in hospitals, emergency departments and long-term care homes. However, those who received a nonphysician-provided palliative home care visit before death represented only half of the decedents who were likely at the end of life. While we expected the proportion of decedents who received palliative home care to be lower among those with longer estimated life expectancies, we found a considerable proportion of individuals in their last 3 to 6 months or 6 to 12 months of life also did not receive any home-based palliative care. Across individuals who were most likely to benefit from palliative care, one of the main contributing factors to whether a home care client received a home visit from either a physician or nonphysician home care provider in their last 6 months of life was a clinician-identified prognosis of having fewer than 6 months to live, whereby individuals who received a home visit were more likely to have had a clinician-identified terminal prognosis than those who did not receive services. In other words, despite the similarity in their clinical characteristics and symptom burden, home care clients who were not given a terminal prognosis by a clinician were much less likely to receive any home visits. This may be an indication that the reduced life expectancies of many older adults — which can be informed using a tool such as RESPECT — are not fully recognized.
RESPECT, as a risk communication tool, was designed for community-dwelling older adults who need care (e.g., from nurses or personal support workers) to live at home and to support earlier identification of their palliative care needs. RESPECT is openly accessible through ProjectBigLife.ca, and its implementation and acceptability as an openly accessible online tool for communicating the risk of death to community-dwelling older adults have been previously evaluated (unpublished data, 2018). To date, the Web-based tool has been used by more than 400 000 users globally.
According to a Canadian Institute for Health Information 2018 report, as many as 89% of people with a life-limiting illness, including frailty, could benefit from palliative care.8 A prognosis of 3 to 12 months has been considered an appropriate time frame for referral to palliative care among oncology experts.20 However, palliative care must be provided at least 3 to 4 months before death for maximal benefits, according to a systematic review of randomized trials of early integration of home and outpatient palliative care.21 Our finding that only half of the individuals with an estimated survival of fewer than 3 months received any palliative home care suggests there are potentially unmet palliative care needs among community-dwelling older adults in Ontario. Furthermore, those who did not receive palliative home care were more likely to have had an inpatient admission, potentially suggesting a lack of access to home-based support. These results reinforce the role of clinicians in identifying older adults who may be in their last 6 months of life as an important component for the receipt of palliative home care, and highlight the value of RESPECT in supplementing clinicians’ assessments of prognosis.
A variety of factors may prevent individuals from accessing palliative care services, despite the benefits that have been shown to be associated with receiving such care. A persistent barrier is the delayed identification of care needs and the late introduction of appropriate support or services.20,21 However, it is often challenging for clinicians to predict survival, and prior research suggests clinicians’ predictions are often overly optimistic. 22,23 Screening and assessment tools, such as RESPECT, can therefore be used to support clinicians’ ability to identify and assess need.24
While RESPECT can be easily implemented and used by both clinicians and patients to support earlier identification of palliative care needs and inform care planning, it cannot address the multitude of pre-existing challenges that currently limit access to early palliative care services once a need has been identified. These include, for instance, the lack of public and professional awareness of the benefits of palliative care;25 lack of service infrastructure; and human resource constraints,26 including lack of primary care providers25 as well as a lack of knowledge and skills in palliative care areas (e.g., assessment and management of pain and symptoms, care coordination, and communication). 27,28 Nonetheless, early identification of those nearing the end of life is an important first step. This is supported by existing literature involving randomized controlled trials of hospitalized patients, which suggests the use of prediction models for triggering palliative care can increase the proportion of palliative care consults and referrals, as well as earlier referrals to palliative care.29
This study offers a unique perspective through the prospective examination of trends in health care service use among home care clients in Ontario. Much of the existing literature uses retrospective methods to examine outcomes of interest, such as health care use, among decedents at various periods before death.10,30–32 While data used in this study are historic, our approach distinguishes this study from others by first estimating the risk of death — and classifying individuals accordingly — before examining individuals’ prospective health care use. In doing so, we gain insights into how we may be able to prospectively identify the health care people will need to increase palliative care for people requiring this type of service.
Limitations
The use of routinely collected health administrative data enabled us to examine the health care utilization pattern of home care clients with different mortality-risk profiles at the population level. While we were able to present the breadth of services provided, administrative data do not capture all pertinent information that could influence a patient’s propensity for receiving home-based care, such as the availability of family members or caregivers to support them in the home. Furthermore, some patients in our study cohort may have died unexpectedly or suddenly, and may not have the opportunity to benefit from earlier interventions. However, the extent of this phenomenon is difficult to assess given limitations of these data.
Conclusion
We found that only half of home care clients with a median survival of fewer than 3 months who died within 6 months of an interRAI Home Care assessment received a palliative home care visit. A substantial proportion of clients likely in their last few months to years of life do not receive any palliative care and continue to be admitted to hospitals and long-term care homes, potentially indicating considerable unmet palliative care needs. Consequently, many are not supported to die in the community, suggesting that their end-of-life care experiences may be misaligned with their preferences. This highlights the value of prognostic models such as RESPECT to support earlier identification of palliative care needs and inform care planning for individuals in their final years of life.
Footnotes
Competing interests: Amy Hsu is an executive lead on the steering committee of the Ontario Centres for Learning, Research, and Innovation in Long-Term Care. Funding for the centres comes from the Ontario Ministry of Health and Ministry of Long-Term Care and is partially administered by the Bruyère Research Institute. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Maya Murmann and Amy Hsu were co-leads in the study design and were responsible for interpreting the results and writing the manuscript. Michael Pugliese was responsible for analyzing and interpreting data and providing critical revisions to the manuscript for its methodological content. Douglas Manuel, Peter Tanuseputro, Carol Bennett, Wenshan Li, and Rhiannon Roberts contributed to the design of this study and provided critical reviews of its clinical and methodological content. All authors reviewed the manuscript, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding: This work was supported by the Canadian Institutes of Health Research (funding reference nos. PHT — 178436 and PJT — 153251) and the Associated Medical Services.
Data sharing: The data set for this study is held securely in coded form at ICES. Although data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at https://www.ices.on.ca/DAS. The full data set creation plan and underlying analytic code are available from the authors on request, with the understanding that the computer programs may rely on coding templates or macros that are unique to ICES and are therefore inaccessible or may require modification.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ontario Ministry of Long-Term Care. The opinions, results, and conclusions reported in this paper are those of the authors and are independent of the funding sources. No endorsement by ICES, the Ontario Ministry of Health, or the Ontario Ministry of Long-Term Care is intended or should be inferred.
- Accepted December 13, 2023.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

