


The sex-based physician compensation gap encompasses within-specialty, between-specialty, and patient-specific inequalities in compensation.
Female physicians and female-dominant specialties are compensated less than their male counterparts; these inequalities are worsened by differences in compensation for services provided to female versus male patients.
A pan-Canadian, standardized, and transparent approach to fee-for-service compensation with an equality lens is needed to address structural inequalities in compensation embedded in the schedule of medical benefits.
The compensation gap between male and female physicians in Canada is well documented. Male physicians receive higher compensation than their female peers across and within specialties, remuneration models, and practice settings — even after accounting for hours worked and the number of patients seen.1 We discuss the multifactorial nature of this compensation gap and the range of interventions required to address the problem fully.
The sex-based physician compensation gap can be understood as 3 inequalities — within-specialty, between-specialty, and patient-specific compensation inequality — each with unique contributors (Figure 1 and Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.231518/tab-related-content). Within-specialty compensation inequality refers to differences in hourly and per-patient payment for male and female physicians delivering the same services. Observational data suggest that differences in payment are at least partly caused by sex-based differences in case-mix,2 referrals for non-procedural consultations, 3 time spent per patient,4 negotiation styles,5 and non-billable administrative tasks.6 Between-specialty compensation inequality refers to differences in compensation between male-predominant and female-predominant specialties for similar work.1 This inequality may be related to the devaluation of a specialty as the proportion of females working in it increases, as seen in other fields,7 and to gendered factors influencing specialty selection by female medical students.8
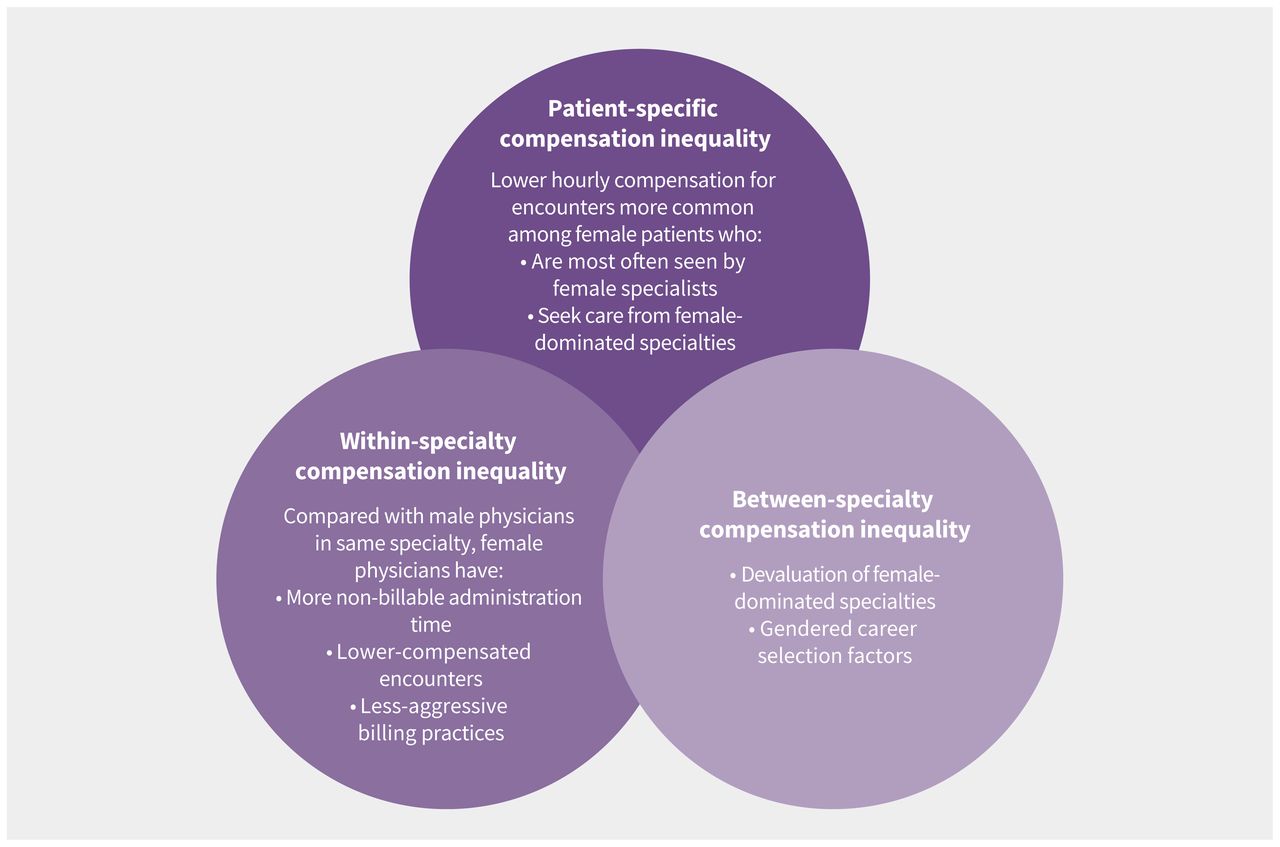
Conceptualization of sex-based compensation inequality, with examples of how within-specialty, between-specialty, and patient-specific compensation inequality may contribute.
Both of these compensation inequalities may be further widened by patient-specific compensation inequality, which refers to differences in compensation for services provided to female compared with male patients. An obvious example of how patient-specific compensation inequality contributes to the between-specialty compensation gap is that procedures performed on female anatomy (most often by gynecologists, a female-dominated specialty) are compensated at a lower rate than those performed on male anatomy (most often by urologists, a male-dominated specialty).9 However, patient-specific inequality also widens the within-specialty gap in surgical specialties; for example, female urologists see a greater proportion of female patients than their male colleagues and female urology patients more often require urodynamic procedures than male urology patients, which are compensated at a lower rate than other urologic procedures.10
About 70% of physician compensation in Canada follows a fee-for-service model, whereby a physician receives a predetermined amount for each medical encounter or procedure performed. A schedule of billing codes is negotiated between provincial or territorial health ministries and their respective provincial medical associations. A common misconception is that no sex discrimination is present in the fee-for-service compensation model since physician sex is not considered in billing codes. However, because female patients are more often cared for by female physicians, regardless of specialty,2 the interaction of between-specialty and patient-specific compensation inequality is particularly important in understanding the compensation gap. This interaction has been termed “double discrimination” and can be interrogated by comparing payment for procedures performed on male reproductive anatomy (e.g., urologic procedures) and female reproductive anatomy (e.g., gynecologic procedures) across male-dominated (urology) and female-dominated (gynecology) specialties. A rigorous comparison of similar urology and gynecology procedure codes in Canada by Chaikof and colleagues9 found that gynecologic procedures were paid, on average, 28% less than matched urologic procedures, with wide variation in this difference across provinces. Although structural discrimination in the schedule of medical benefits is not the only contributor to the compensation gap, the study suggests that the provincial and territorial schedule of medical benefits contributes to between-specialty and patient-specific compensation inequality.9
Unlike sociocultural or biologic factors, restructuring the schedule of medical benefits is within the purview of governments and provincial medical associations. Further, this approach is likely acceptable to all stakeholders despite potential skepticism about the existence of or contributors to the sex-based compensation gap. Achieving a more equal distribution of the value of billing codes for male and female anatomic procedures based on technical complexity would not require all to agree that a compensation gap exists or that it exists because of systemic and interpersonal sexism rather than personal choices. Rather, stakeholders must acknowledge only that all physicians deserve equal pay for similar work, in keeping with Canada’s Human Rights Act, which prohibits sex-or gender-based discrimination in pay.
A central hurdle in renegotiating the schedule of medical benefits is defining “same work.” Identifying matched codes for certain specialty types is challenging, particularly for nonprocedural specialties or very subspecialized surgeries. Similarly, differences in female and male anatomy mean that sex-specific procedures may not be easily compared. A lack of trust between provincial governments and medical associations may adversely affect negotiations about the relative value of services.
Despite challenges, a method to assess and eliminate sex-based discrimination in fee-for-service compensation is needed. Relative valuation calculations, where the difference in compensation for 2 similar procedures or encounter types is divided by the total compensation for both, may identify billing codes that deserve further attention. Medicare in the United States and publicly funded health care in France have standardized fee-for-service compensation based on objective measures such as procedure duration, technical skill, and overhead costs, which demonstrates the feasibility and acceptability of this approach.11
A pan-Canadian, standardized, and transparent approach to fee-for-service compensation with an equality lens is clearly needed. One way forward would be to develop and maintain a national system that analyzes and transparently reports variations in matched billing codes between provincial schedules of medical benefits to identify outliers that may need further consideration. This may alert provincial and territorial governments and medical associations to billing codes that may be relatively over- or undervalued. Evidence from business and policy literature suggests that compensation transparency can reduce sex-based inequality.12 A transparent and non-negotiable standardized compensation process reduced between-specialty compensation inequality in a multicentre study from the US.13
Fee-for-service billing codes can perpetuate compensation inequalities. These inequalities highlight a larger concern about how female patients are valued and how value is ascribed to work done by physician groups who are mostly female. Work is needed to adopt evidence-informed processes that can address sex-based compensation inequality across Canada.
Footnotes
Competing interests: Shannon Ruzycki reports research funding from Alberta Innovates, the Canadian Institutes of Health Research (CIHR), and the University of Calgary Office of Health and Medical Education Scholarship, as well as honoraria from the University of Ottawa and the University of Alberta. Natalie Yanchar reports research funding from CIHR; she is deputy department head of the Department of Surgery, University of Calgary. Oluwatomilayo Daodu reports research funding from the Cumming School of Medicine Clinical Research Fund, the University of Calgary Office of Health and Medical Education, the University of Calgary Vice President (Research) Catalyst Grant, the Alberta Children’s Health Research Institute, and the Social Sciences and Humanities Research Council. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Saud Sunbar, Natalie Yanchar, and Oluwatomilayo Daodu conceptualized this work. Shannon Ruzycki and Maede Ejaredar contributed to the analysis. Shannon Ruzycki and Oluwatomilayo Daodu drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

