


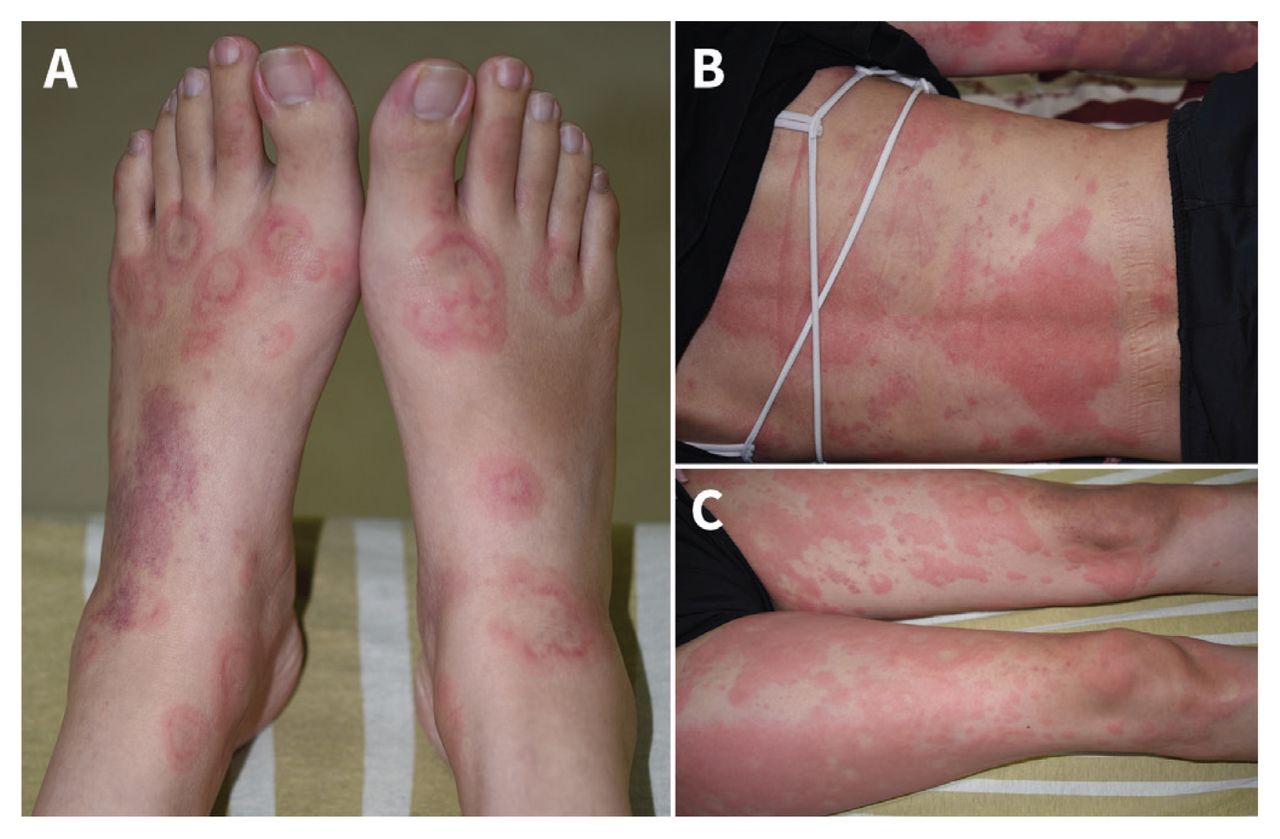
A 29-year-old woman presented to the emergency department with dyspnea and palpitations, as well as a pruritic and painful rash that had developed over the previous 5 days. Her temperature was 38.6°C, heart rate was 174 beats/min and respiratory rate was 24 breaths/min. We observed a diffusely enlarged thyroid gland as the patient swallowed and annular, erythematous–violaceous plaques on her face, trunk and extremities (Figure 1). Laboratory investigations showed a free tetraiodothyronine level of 2.37 (normal 0.70–1.48) ng/dL, a thyroid-stimulating hormone level of less than 0.008 (normal 0.35–4.94) μIU/mL, an antithyroid peroxidase antibody level of 67.8 (normal < 5.6) IU/mL, a thyroid-stimulating hormone receptor antibody level of 7.5 (normal < 1.75) IU/L and a complement C3 level of 75.6 (normal 90–180) mg/dL. Skin biopsy from a lesion on the patient’s abdomen showed perivascular infiltrates with numerous neutrophils, nuclear dust, scattered eosinophils and erythrocyte extravasations, consistent with leukocytoclastic vasculitis (Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.211926/tab-related-content).

Urticarial vasculitis in a 29-year-old woman with Graves hyperthyroidism. (A) Multiple annular, erythematous–violaceous, urticarial plaques with petechiae dorsally on both feet. (B) Erythematous, wheal-like plaques with confluence on the patient’s back and purpura on her arms. (C) Widespread erythematous, urticarial plaques with purpuric change on both lower extremities.
We diagnosed hypocomplementemic urticarial vasculitis associated with Graves hyperthyroidism. We excluded other conditions associated with urticarial vasculitis, including viral hepatitis, autoimmune connective diseases, cryoglobulinemia and hematologic malignant diseases.1,2 Our patient’s skin lesions resolved after 2 weeks of treatment with methylprednisolone (40 mg/d), propylthiouracil (200 mg/d) and propranolol (30 mg/d). She had no recurrence of urticarial vasculitis in the 3 months after treatment; her thyroid hormone levels remained normal using a tapered dose of propylthiouracil (50 mg/d).
Urticarial vasculitis presents with urticarial lesions and histopathologic features of cutaneous leukocytoclastic vasculitis. The lesions are more purpuric, are longer lasting (> 24 h) and have a tendency to burn, compared with other causes of acute urticaria such as infection or allergy to food.3 The association of urticaria with thyroid autoimmunity is widely recognized.1–3 In a retrospective study, 42% of patients with urticarial vasculitis had abnormal antithyroid antibodies, a 15-fold higher odds than patients with chronic spontaneous urticaria. 3 Clinicians should consider important mimics in their differential, such as antithyroid medications, which are known to induce vasculitis associated with antineutrophil cytoplasmic antibodies.4
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article extras
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

