


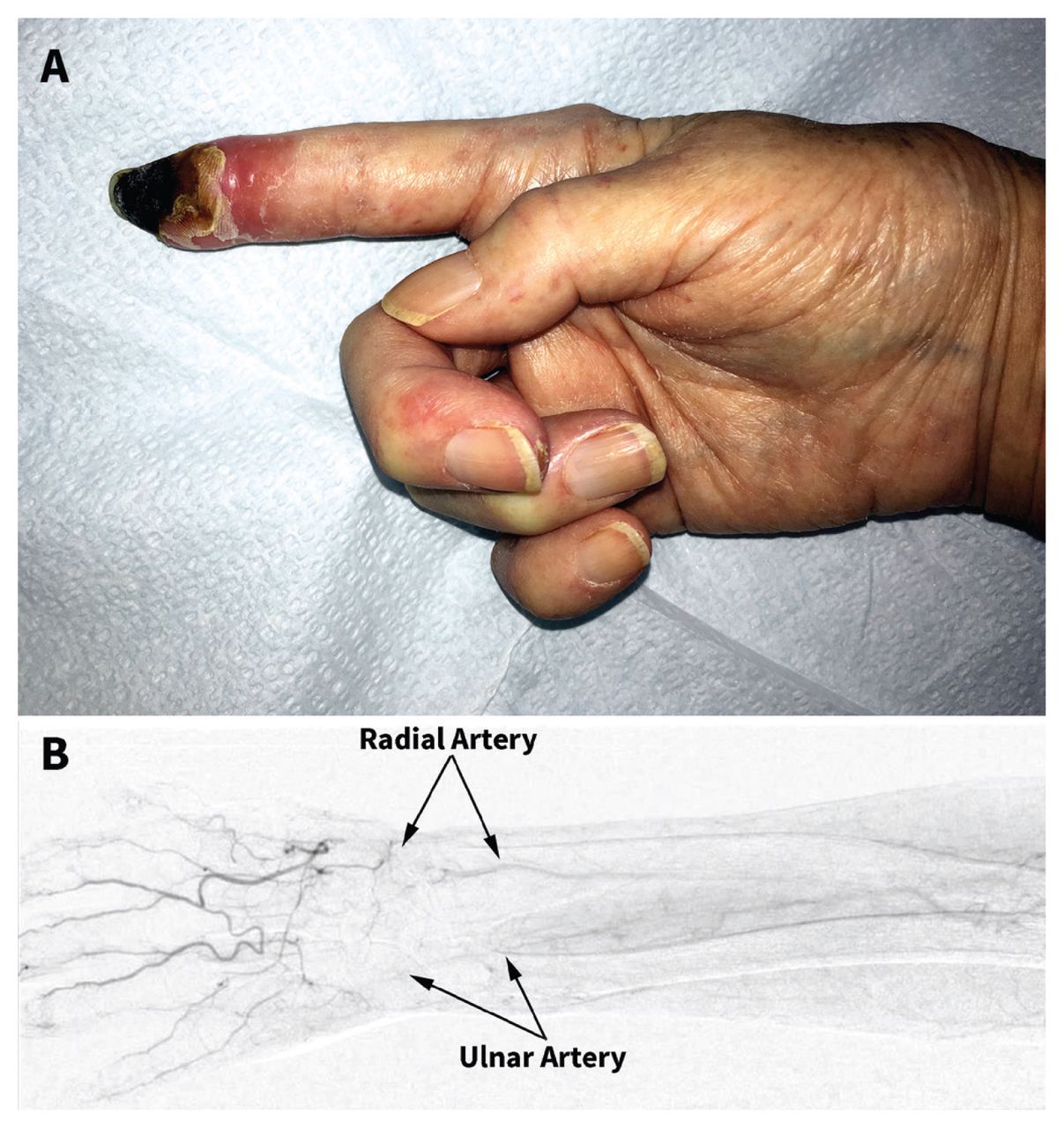
A 68-year-old woman presented to our clinic with intractable pain, pallor and dry gangrene at the tip of her right index finger (Figure 1A). She had a history of systemic sclerosis, including well-controlled Raynaud phenomenon, dysphagia, interstitial lung disease, complete heart block and progressive cardiomyopathy. She had no previous episode of critical digital ischemia (i.e., severe pain, digital ulceration or gangrene). Six weeks earlier, she had been admitted to the hospital with acute hypoxic respiratory failure and required multiple sampling via her right radial artery.

(A) Digital tip dry gangrene (black discoloration) of the right index finger of a patient with scleroderma. (B) Angiography showed narrowing of the right radial artery and occlusion of the right ulnar artery at the wrist with the reconstitution of a palmar arch, where the arteries were also moderately diseased.
Angiography showed narrowing of the patient’s right radial artery and occlusion of the right ulnar artery (Figure 1B). We attributed her digital gangrene to occlusion of the right ulnar artery from scleroderma macrovasculopathy and radial artery injury secondary to multiple punctures. Mittens, air-activated hand warmers, nifedipine, topical nitroglycerine and sildenafil were ineffective at alleviating her symptoms. We treated her with intravenous heparin, then warfarin. Three months later, a distal phalangeal amputation was performed.
About 10% of the general population1 and one-third of patients with scleroderma2 have ulnar arterial occlusion. Age older than 50 years, male sex and repetitive palmar trauma related to occupational exposure are risk factors, and the dominant side is more commonly affected.1 A modified Allen test3 can be performed at the bedside to assess hand circulation (sensitivity 73% and specificity 97%4) before radial arterial sampling for any patient, in particular those with scleroderma (Box 1). An arterial duplex scan is the gold standard but is often unavailable.
Modified Allen test
Elevate the hand and ask the patient to clench the fist for 30 seconds. Next, occlude the ulnar and radial arteries with your fingers. Ask the patient to unclench the fist of the elevated hand; the palm and the fingers should appear blanched. Then, release the pressure over the ulnar artery while maintaining the pressure over the radial artery. The colour to the palm and fingers should return within 15 seconds, indicating a normal ulnar arterial patency. Failure of the colour to return implies inadequate ulnar arterial supply.
Acknowledgement
The author thanks the patient’s husband (the patient is deceased) for providing written permission to share her information.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The author has obtained spousal consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article extras
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

