


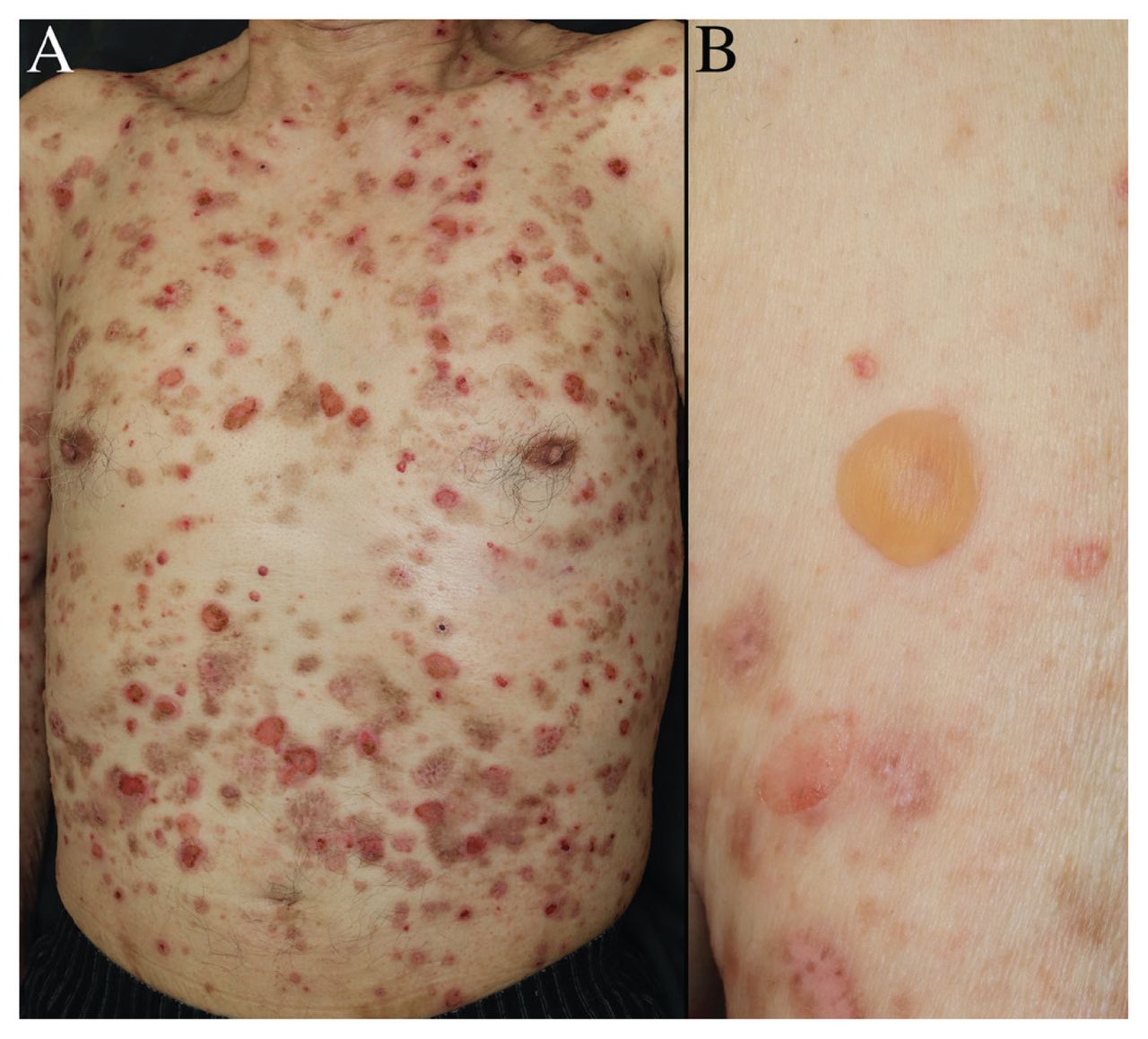
An 86-year-old man with a 7-month history of widespread pruritic bullae was referred to our dermatology clinic by his family physician. Physical examination showed tense bullae on his trunk and extremities, as well as areas of erosion and crusting where bullae had ruptured (Figure 1). We did not observe any mucosal lesions. Three years earlier, he had started teneligliptin for treatment of type 2 diabetes mellitus.

Photographs of a 86-year-old man with bullous pemphigoid. (A) Bullous lesions, and erosion and crusting at sites of ruptured bullae, on the trunk. (B) Tense bulla without an inflammatory base on the patient’s left upper limb.
Bloodwork showed a leukocyte count of 6900 (normal 3300–8600) μL with 8% (normal 0%–8%) eosinophils. Tests for antibodies to the NC16A domain of the bullous pemphigoid antigens 180 (BP180) and 230 were negative. A skin biopsy showed subepidermal blister formation (Appendix 1, Figure 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.211933/tab-related-content), and direct immunofluorescence showed a linear staining pattern with immunoglobulin G in the basement membrane. We diagnosed bullous pemphigoid associated with use of a dipeptidyl peptidase-4 (DPP-4) inhibitor. We stopped teneligliptin and treated the patient with oral prednisolone 40 mg/d for 2 weeks, followed by weekly taper, which led to a complete resolution of the rash within 2 weeks.
Bullous pemphigoid is an autoimmune blistering disease, characterized by severe pruritis, tense bullae and edematous erythema. 1 Dipeptidyl peptidase-4 inhibitors are commonly used to treat diabetes, and are associated with development of noninflammatory bullous pemphigoid, with an incidence of 0.42 per 1000 person-years.1–3 Reported risk factors for development include male sex, white race and use of vildagliptin or linagliptin.1,2 Bullous pemphigoid usually begins several months to years after the initiation of a DPP-4 inhibitor.3 Unlike inflammatory bullous pemphigoid, bullous pemphigoid associated with DPP-4 inhibitors tends to present without serious urticaria or erythema at the base of the lesions, and patients are often seronegative for NC16A domain of BP180, as with our patient.3,4 Stopping the DPP-4 inhibitor results in complete resolution of symptoms in about one-third of patients.2 Patients who are still symptomatic should be referred to a dermatologist, who may treat with corticosteroids or tetracyclines.
Acknowledgement
The authors thank James R. Valera for his assistance in editing the manuscript.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue
{kind=link}
Article extras
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

