


Polycystic ovarian syndrome (PCOS) is a chronic disorder associated with infertility; miscarriage; adverse pregnancy outcomes; and cardiovascular, metabolic, psychological and neoplastic risks.
Diagnosis of PCOS can be made based on the presence of any 2 of menstrual irregularities, clinical or biochemical hyperandrogenism or polycystic ovarian morphology on transvaginal ultrasonography.
Treatment of PCOS may target anovulation, androgen excess, hyperinsulinemia and weight management.
Patients with PCOS should have regular monitoring of their body mass index, blood pressure and metabolic parameters, and should be regularly screened for depression, anxiety and obstructive sleep apnea.
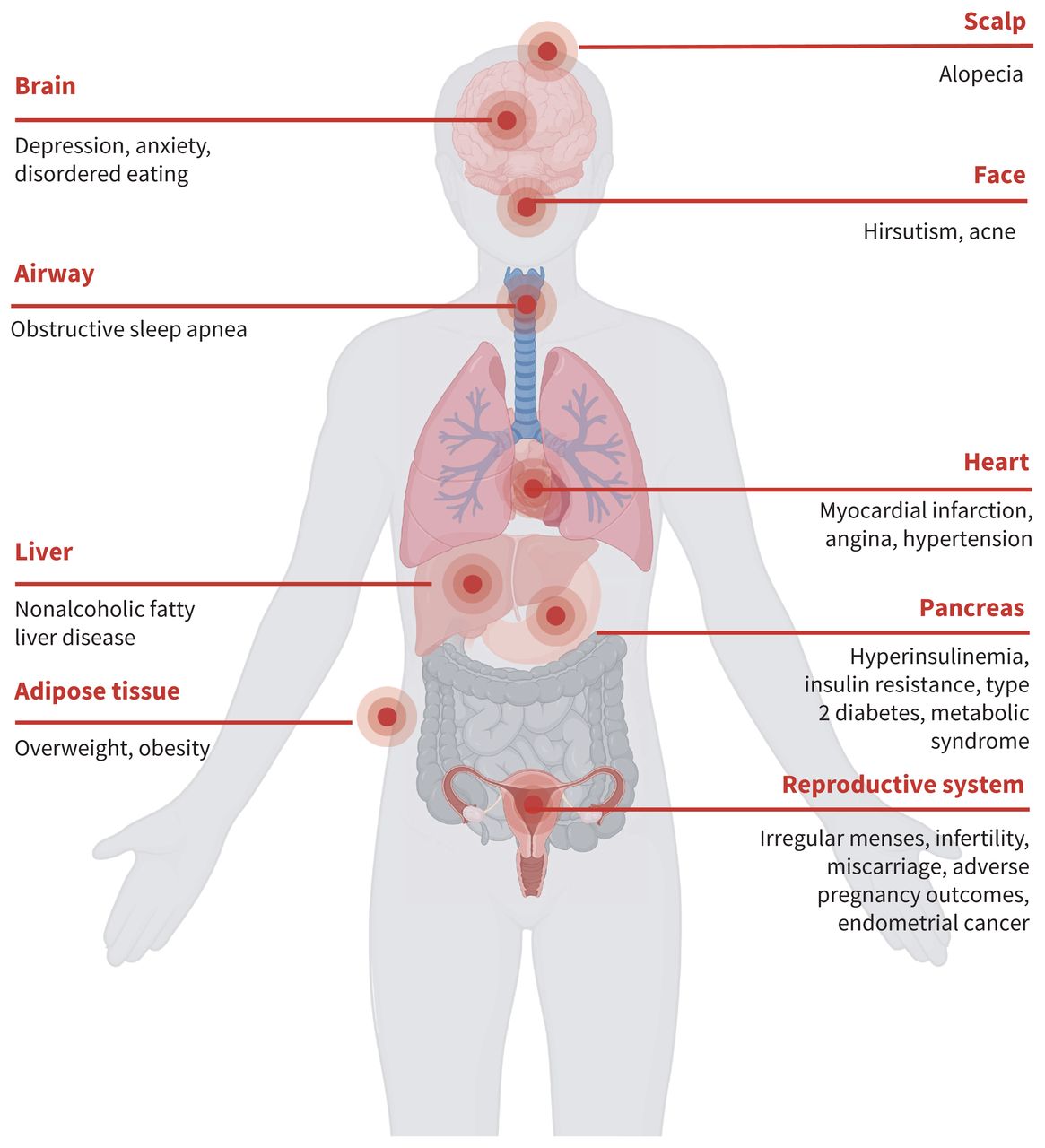
Polycystic ovarian syndrome (PCOS) causes irregular menstrual cycles and symptoms of hyperandrogenism and affects 10% of females (Figure 1).1 Symptoms most often begin between the ages of 18 and 39 years, but diagnosis and treatment of PCOS are often delayed or patients remain undiagnosed.1,2 People with PCOS are more likely to be overweight or obese (53%–74%) than those without the condition, and higher body mass index (BMI) is associated with more severe symptoms of PCOS.3–5 Patients with PCOS also have higher rates of adverse reproductive, cardiovascular, psychological, metabolic and neoplastic outcomes than the general female population.3,6 Early diagnosis of PCOS allows for identification and treatment of associated conditions such as hypertension, diabetes, obstructive sleep apnea, depression and anxiety. We review evidence on the pathophysiology, diagnosis and management of PCOS from guidelines and other relevant articles (Box 1).
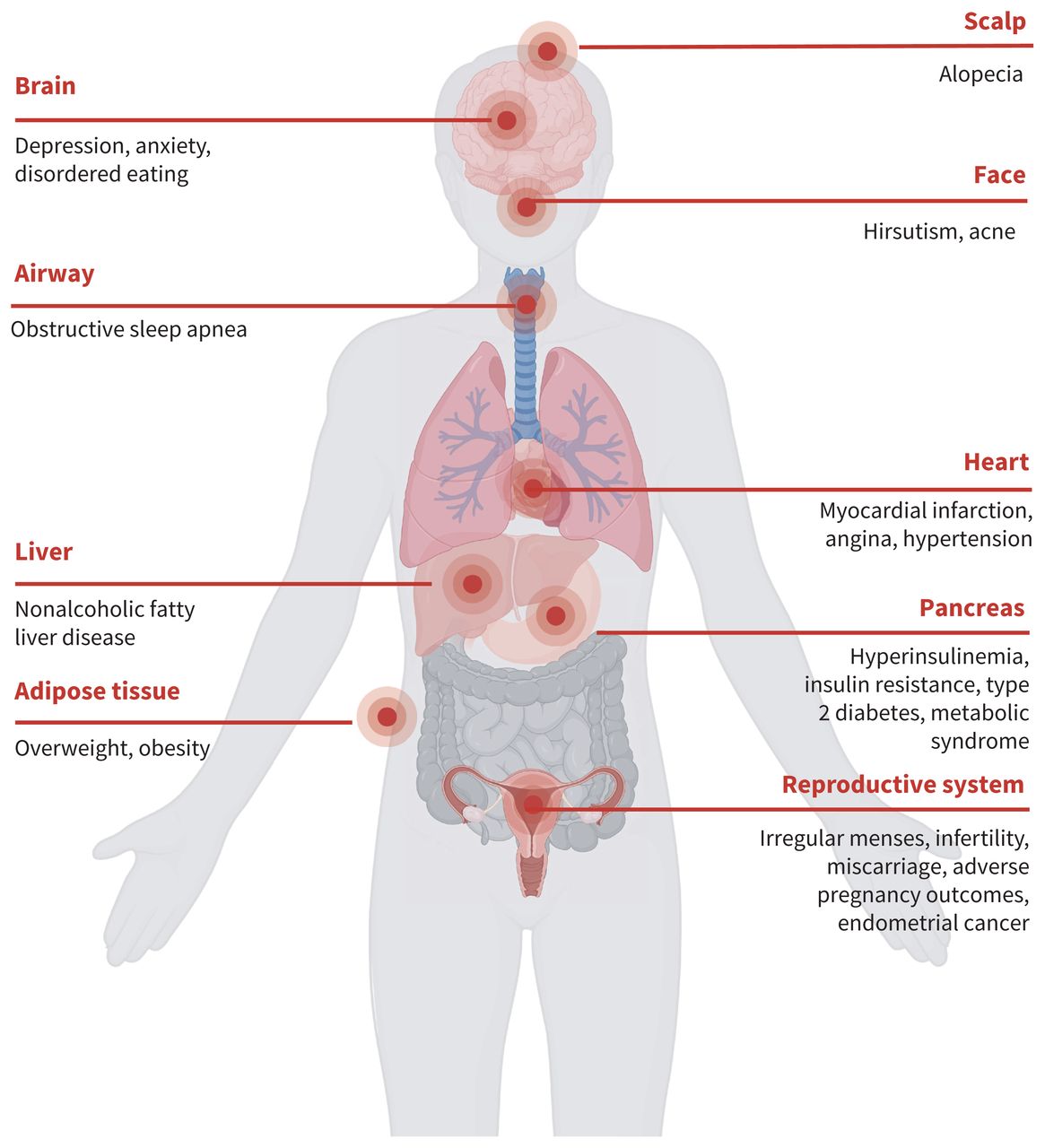
Health impacts associated with polycystic ovarian syndrome. Created with BioRender.com.
Box 1: Evidence used in this review
We drew on the international guideline on the management of polycystic ovarian syndrome (PCOS) published by the European Society of Human Reproduction and Embryology and the American Society for Reproductive Medicine in 2023 and the hirsutism guideline published by the Endocrine Society in 2018.1,3,7 We also searched articles in PubMed from 2018–2023 using the terms “PCOS,” and “polycystic ovarian syndrome.” We considered all articles and further searched reference lists of relevant articles to find other articles of interest.
What is the pathophysiology of PCOS?
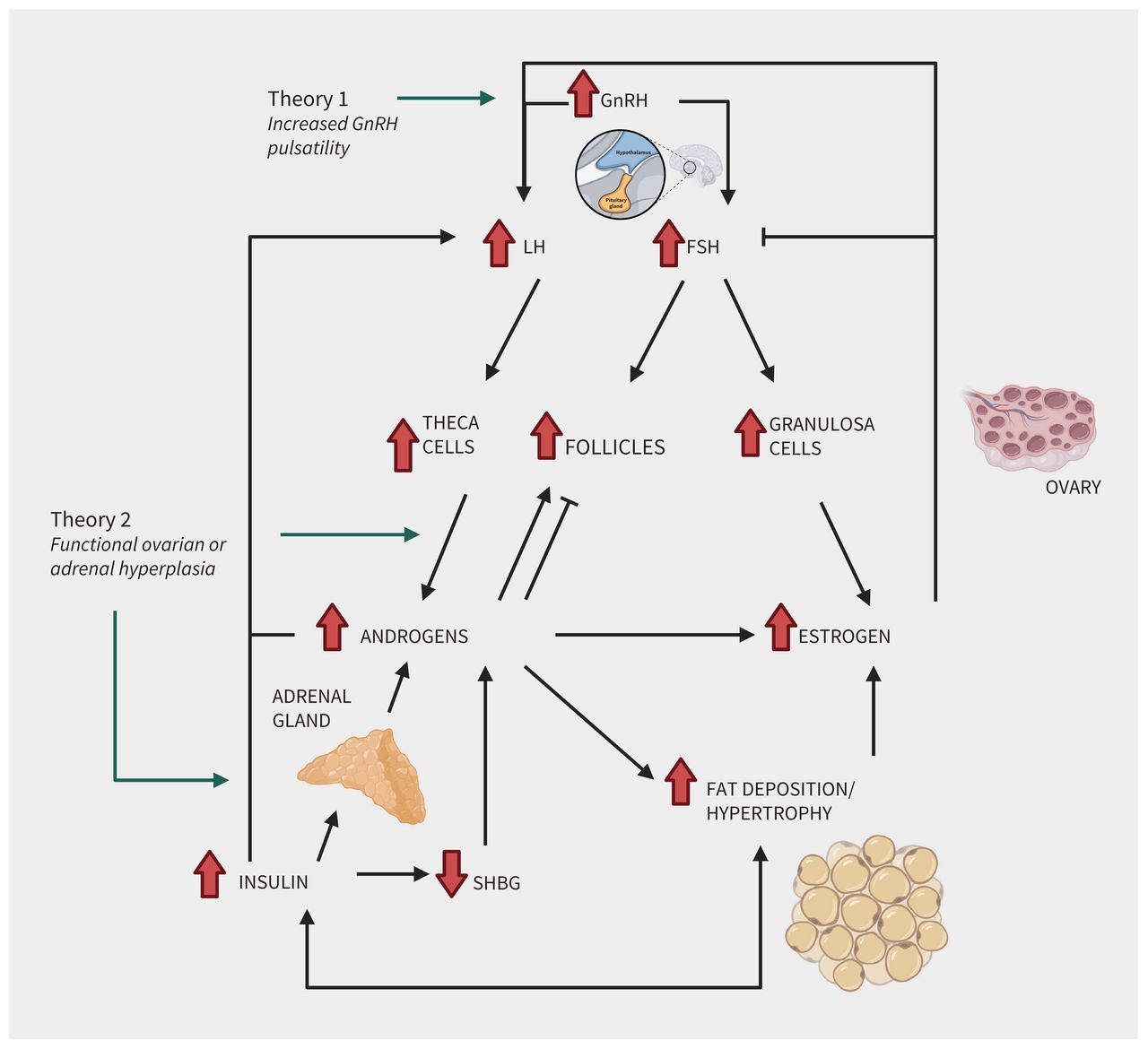
The pathophysiology of PCOS is complex and poorly understood. Hyperandrogenism and hyperinsulinemia underpin the clinical symptoms, diagnosis and treatment targets of PCOS. Clinical phenotypes vary widely. Whether the presence of immature ovarian follicles, characteristic of PCOS, precedes hyperandrogenism, hyperinsulinemia and their associated clinical symptoms or vice versa remains unclear (Figure 2).8
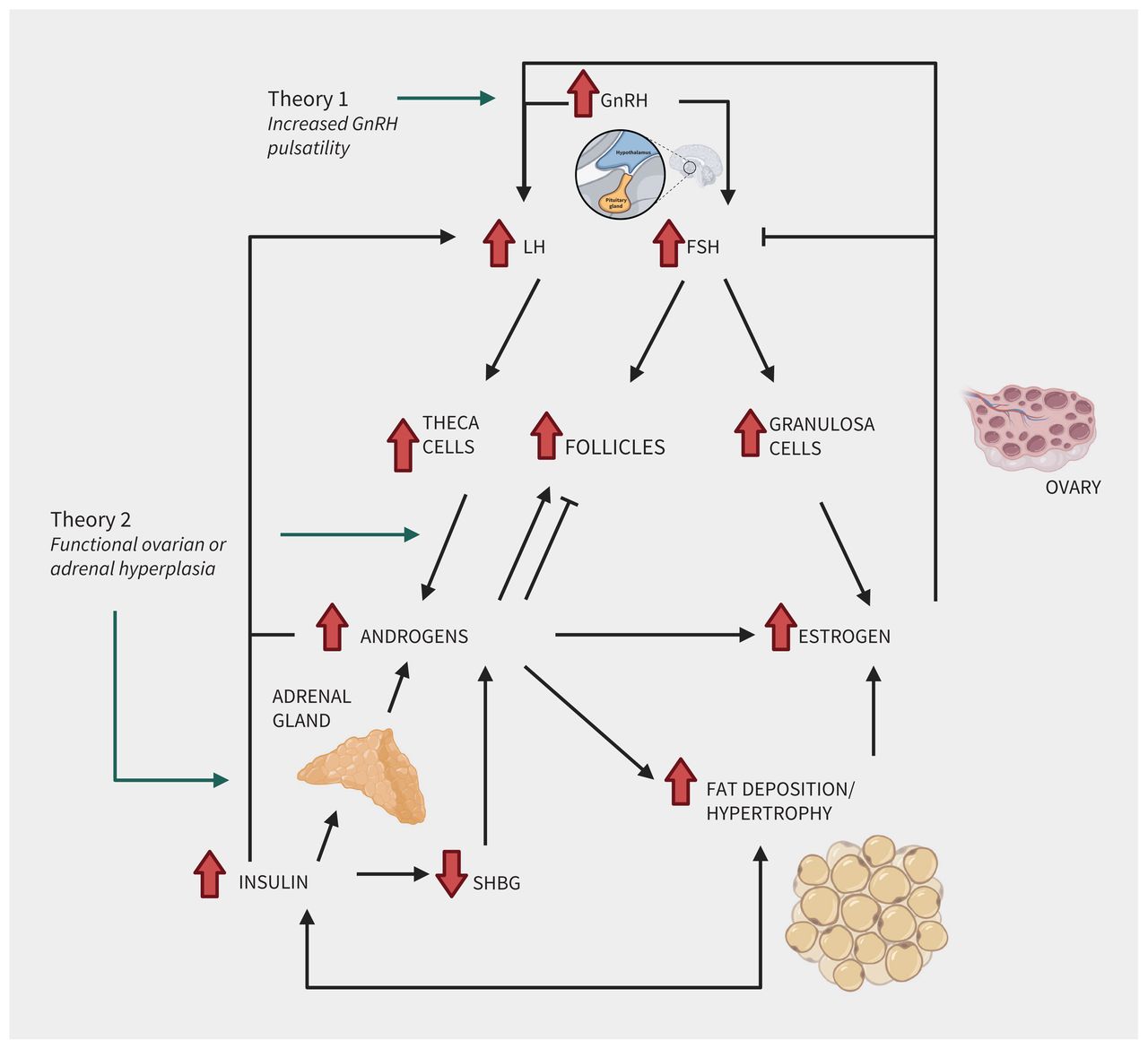
Two theories of the pathophysiology of polycystic ovarian syndrome (PCOS). The 2 main defining pathophysiological mechanisms of PCOS are hyperandrogenism and hyperinsulinemia; this relationship has been described and one perpetuates the other, but the exact mechanisms are not fully elucidated. The 2 main theories that are postulated include increased gonadotropin-releasing hormone (GnRH) pulse frequency (theory 1) and functional ovarian or adrenal hyperandrogenism (theory 2). Gonadotropin-releasing hormone stimulates release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) from the anterior pituitary. At the ovary, LH acts on theca cells to produce androgens; FSH acts on granulosa to produce estrogens. Estrogen has negative feedback mechanisms to FSH production. Both androgens and estrogen stimulate LH production. Ovarian release of androgens may also be functional. Hyperandrogenism, as well as FSH and LH stimulation, stimulates both follicular development and atresia leading to the classic multifollicular appearance of the ovaries on ultrasonography. Androgens may also be overproduced by the adrenal glands, which may be further driven by insulin. Both hyperinsulinemia and hyperandrogenism are postulated to be worsened by and drive adipose tissue deposition. Created with BioRender.com.
Two theories for why hyperandrogenism occurs in PCOS have been proposed.8 The first theory, called the altered gonadotropin secretion theory, postulates that increased gonadotropin-releasing hormone (GnRH) pulse frequency leads to excessive levels of luteinizing hormone (LH) and slightly elevated levels of follicle-stimulating hormone (FSH).9–11 Elevated LH stimulates androgen production from theca cells, while elevated FSH stimulates follicular development and excess estrogen production.10,11 The second theory, called the functional ovarian or adrenal hyperandrogenism theory, postulates that hyperandrogenism originates from dysregulated steroidogenesis at the level of the ovary or adrenal gland.8
Elevated androgens support follicular recruitment while also inducing follicular atresia.8,10,12 This ultimately leads to the classic appearance of multifollicular ovaries (or polycystic ovaries) on transvaginal ultrasonography.
Hyperinsulinemia is thought to have multiple effects including elevating LH, decreasing sex hormone–binding globulin (SHBG), increasing conversion of androstenedione to testosterone and reducing LH desensitization at the level of the ovary.9,10 Hyperinsulinemia leads to an increase in visceral adipose tissue deposition and hypertrophy. Hyperandrogenism may also lead to increased visceral adiposity. Obesity worsens symptoms of PCOS but the prevalence of PCOS rises only slightly with increasing BMI, suggesting it is not the main cause of PCOS.5,10,13
What symptoms do patients with PCOS describe?
Patients with PCOS often have menstrual cycle irregularities with or without features of hyperandrogenism, which include hirsutism, acne and female-pattern alopecia (overall thinning with maintenance of hairline).1 Before a diagnosis of PCOS can be made, other causes for these phenomena must be excluded. These alternative causes include hyperprolactinemia, thyroid dysfunction, non-classic congenital adrenal hyperplasia, Cushing syndrome, ovarian tumours or adrenal tumours. A detailed history is the first step to differentiating among potential causes of a patient’s symptoms.
Symptoms suggestive of PCOS
Patients with PCOS typically present with irregularities in the frequency of their menstrual cycle, suggestive of anovulation. Menstrual cycle patterns among patients with PCOS can fluctuate through a patient’s lifetime, ranging from amenorrhea to regular ovulatory cycles. Clinicians should determine whether the patient has a family history of PCOS, dyslipidemia, hypertension or diabetes, as PCOS has a heritable component.3
The androgenic symptoms of PCOS — such as acne, hirsutism and female-pattern alopecia — develop gradually. Hirsutism, which is the symptom most predictive of biochemical hyperandrogenisim, can be assessed objectively using the Ferriman–Gallwey score, although the clinical utility of this scoring system is limited as patients will often engage in hair removal before assessment.1 Thus, subjectively distressing hair growth can be adequate to consider treatment.1
Clinical features suggestive of other diagnoses
Other causes of both hyperandrogenism and menstrual cycle irregularities that can mimic PCOS include non-classic congenital adrenal hyperplasia and Cushing syndrome. Although non-classic congenital adrenal hyperplasia is clinically indistinguishable from PCOS, many patients with Cushing syndrome will have other features such as violaceous striae, weight gain with central fat deposition and dorsal fat pad, easy bruising and proximal muscle weakness.
Intermenstrual bleeding and heavy regular menstrual bleeding are not usually associated with PCOS; infectious or structural causes of heavy bleeding such as fibroids, polyps or adenomyosis should be considered. Associated symptoms, such as hot flashes presenting in the context of new menstrual cycle irregularities, are more suggestive of premature ovarian insufficiency.
Patients with thyroid dysfunction and hyperprolactinemia may have additional symptoms; skin or hair changes or hot or cold sensitivity often accompany thyroid dysfunction, and galactorrhea, headaches, visual changes are features of hyperprolactinemia. A thorough review of medications that may cause hyperprolactinemia or hyperandrogenism should also be undertaken. Severe, sudden onset of virilizing symptoms (e.g., clitoromegaly, voice deepening, male-pattern balding) are more suggestive of an androgen-secreting tumour originating from the adrenal glands or ovaries.7
How is PCOS diagnosed?
The Rotterdam criteria are the most widely accepted criteria for diagnosis of PCOS (Box 2).1 As PCOS is considered a diagnosis of exclusion, diagnostic testing is required for patients presenting with symptoms, although the results of this testing may be normal. Suggested investigations are included in Box 3. An interpretation of test findings can be found in Table 1. If a patient has a concomitant disorder, such as hypothyroidism, the concomitant disorder should be treated and the patient should be reassessed to determine whether the patient has PCOS.
Box 2: Rotterdam criteria1
Polycystic ovarian syndrome is diagnosed when 2 out of 3 of the following criteria are met and other diagnoses are excluded:
Irregular cycles (if > 3 yr post-menarche, > 35 d apart or < 21 d apart; < 8 menstrual cycles per year; or > 90 d for any 1 menstrual cycle)
Clinical hyperandrogenism (acne, hirsutism, alopecia) or biochemical hyperandrogenism
Polycystic ovarian morphology on transvaginal ultrasonography or high antimüllerian hormone*
↵* Optional if clinical criteria are not met; antimüllerian hormone used as an alternative to transvaginal ultrasonography, but should not be used in adolescents.
Box 3: Suggested initial investigations for patients presenting with menstrual irregularities or clinical hyperandrogenism
Tests should be completed in early follicular phase (day 2–4) in non-amenorrheic patients
Prolactin
Thyroid-stimulating hormone
Luteinizing hormone, follicle-stimulating hormone and estradiol
β-human chorionic gonadotropin (β-hCG)
17-hydroxyprogesterone (17-OHP)
Total testosterone, calculated free testosterone or free androgen index with or without androstenedione, dehydroepiandrosterone sulfate
Transvaginal ultrasonography or antimüllerian hormone*
↵* Only applicable if patient is at least 8 years from menarche.
Initial investigations and differential diagnoses for polycystic ovarian syndrome
Biochemical hyperandrogenism is found in 60% of patients with PCOS and can be assessed using total testosterone, calculated free testosterone, dehydroepiandrosterone sulfate (DHEA-S) and androstenedione.1 If feasible, testing for these androgens should be done in a step-wise fashion, with total testosterone and calculated free testosterone or the free androgen index evaluated first. If these initial investigations are normal, then DHEA-S and androstenedione levels should be tested.1 Androgen levels are only marginally elevated in PCOS; marked elevations should prompt further investigation for androgen-secreting tumours.1 Androgen levels cannot be measured reliably while a patient is on combined hormonal contraceptives (CHCs) because of the elevation in SHBG and altered gonadotropin-dependent androgen production, resulting in falsely lowered values.1 If a patient meets 2 of 3 Rotterdam criteria, this satisfies criteria for PCOS diagnosis without need for laboratory confirmation of elevated androgens. If laboratory confirmation is necessary, CHCs must be stopped for 3 months before measuring androgens.16
Polycystic ovarian morphology on transvaginal ultrasonography (≥ 20 follicles or an ovarian volume ≥ 10 mL in at least 1 ovary) may be an additional criterion if clinical or laboratory criteria are not met.1,12,17 Transabdominal ultrasonography can be used as an alternative with different thresholds (≥ 10 follicles or an ovarian volume ≥ 10 mL in at least 1 ovary).1 The requisition should indicate the clinical concern for PCOS so that an antral follicle count is performed. Normal follicle numbers per ovary can overlap based on age and polycystic ovarian morphology; the normal mean follicle number is 8 among reproductive-aged females, with a mean volume of 6.1 mL.1,18 Polycystic ovarian morphology may be present in as many as 25% of healthy females and is considered a variant of normal.19 Patients should be counselled that cysts are immature follicles, which is a normal finding in all ovaries; the number of follicles is what indicates polycystic ovarian morphology. An incidental finding of polycystic ovarian morphology should prompt the clinician to inquire about irregular menstruation, acne, hirsutism and alopecia, and targeted laboratory evaluation for biochemical hyperandrogenism can also be considered.
The serum anti-müllerian hormone level is also a marker of follicle number. A recent meta-analysis suggests an appropriate threshold for PCOS diagnosis may be an anti-müllerian level of 34.2 pmol/L.15 Values and thresholds are highly dependent on age and laboratory measurement.1 Although the anti-müllerian hormone level can used as an alternative to transvaginal ultrasonography, it is not widely available in laboratories in Canada and is not covered by most provincial health plans.
How are the clinical manifestations of PCOS managed?
Patients with PCOS often request treatment for cycle irregularity, heavy bleeding, acne or hirsutism, and weight management (Table 2).
Weight loss
Among patients who are overweight or obese, weight loss of 5%–10% can help to reduce the severity of symptoms, including menstrual cycle irregularity, acne, hirsutism and alopecia.16,22 No specific diet or exercise recommendations for PCOS are available, and clinicians should be particularly sensitive to weight stigma as patients with PCOS are at risk of dysmorphic body image and disordered eating.1
Combined hormonal contraceptives
Combined hormonal contraceptives are first-line medical treatment options for cycle regulation and hirsutism or acne. No evidence demonstrates the superiority of 1 form of CHC over another in minimizing symptoms and, thus, guidelines cannot recommend which to choose.1,7 Several mechanisms are involved when treating hyperandrogenism with CHCs; the estrogenic component increases SHBG, which decreases the amount of free testosterone, and both the estrogen and progestin provide negative feedback mechanisms to pituitary LH production and thus decrease production of LH-induced ovarian androgen.23
Many patients specifically desire cycle regularity, although this is not medically necessary provided cycles are fewer than 90 days apart. Cycle irregularity may be associated with heavy bleeding. Combined hormonal contraceptives are first-line agents that provide predictable bleeding patterns. When estrogen is contraindicated or not tolerated, progestin-only methods include oral and injectable progestins, the levonorgestrel intrauterine device and the etonogestrel subdermal implant. Oral progestins can be used cyclically (i.e., 3 wk on and 1 wk off) or in rescue fashion (i.e., short course taken after > 90 d amenorrhea) to induce regular withdrawal bleeding. Continuous use of progestins will likely result in amenorrhea. Patients should be reassured that this is a normal outcome with this medication and should not be confused with oligomenorrhea in untreated PCOS. The levonorgestrel intrauterine device and the etonogestrel subdermal implant may provide patients with endometrial protection, as well as less menstrual pain and bleeding, but may not allow for predictability in menstrual bleeding. Many progestins have high androgenic activity and may worsen clinical hyperandrogenism.7
When amenorrhea exceeds 90 days, endometrial protection is critical. The risk of endometrial cancer is 2–6 times higher among people with PCOS than the general population and often presents before menopause.1 Patients with prolonged amenorrhea should be offered CHCs or progestins to maintain a nonproliferative endometrial lining (Table 2). An endometrial biopsy should be considered for all patients with amenorrhea exceeding 90 days, especially if this occurs frequently.24
Nonhormonal medications
Some patients are not candidates for CHCs or prefer not to be on a hormonal medication. Metformin, an insulin sensitizer, can be used as a nonhormonal alternative for PCOS by promoting modest weight loss and reducing insulin levels, which may subsequently have an impact on cycle regularity and hyperandrogenism. 1 A meta-analysis of 22 randomized control trials (RCTs) of metformin for treatment of PCOS found a reduction in BMI (−0.53), testosterone (−13.36 ng/dL) and fasting glucose (−2.39 mg/dL).1 Subgroup analyses demonstrated that metformin lowered BMI, fasting glucose and total and low-density lipoprotein cholesterol among patients with BMI greater than 25, while the free androgen index and fasting insulin were lowered among patients with a BMI less than or equal to 25.1 The efficacy of metformin in reducing clinical features of PCOS remains uncertain. However, given the improvements in metabolic markers, metformin should be considered in patients with PCOS and a BMI greater than 25.1
Metformin has been compared with CHCs in 22 RCTs.1 Between the 2 treatments, no statistically significant differences were shown for weight, BMI or hirsutism, with very low certainty of evidence. Compared with metformin, CHCs did significantly improve menstrual irregularities, with moderate certainty of evidence. Compared with CHCs, insulin and cholesterol levels were improved with metformin with low to very low certainty of evidence. 1 The addition of metformin to CHCs can be considered in patients with PCOS in high metabolic risk groups, which includes those with a BMI greater than 30, those with impaired glucose tolerance, ethnic groups with high metabolic risk factors and those with other diabetes risk factors.1
Inositol is an over-the-counter supplement that can be considered in management of PCOS. It belongs to the vitamin B complex group and is involved in many signalling cascades, including downstream of FSH and insulin. It may have a role in improving insulin sensitivity.1,20 A recent meta-analysis showed that inositol, in particular myo-inositol, reduced BMI (mean difference 0.45 kg/m2) compared with placebo.20 Cycle normalization was higher in the inositol group (relative risk [RR] 1.79). Myo-inositol has minimal adverse effects, although more studies are needed to further support this. Furthermore, as inositol is a supplement, there is no regulation of what is commercially available to consumers and thus it must be used with caution.1,20
Anti-androgen agents
Anti-androgen agents can be considered for patients with clinical hyperandrogenism after 6 months of CHCs with no improvement or in those with contraindications for CHCs. Medical treatment of hirsutism can reduce new hair growth but cannot reverse hair growth that was previously established.7 Only external hair removal techniques such as mechanical laser and light therapy (i.e., laser removal) can be used for previous hair growth. Addition of topical eflornithine may improve outcomes of mechanical laser and light therapy.7
Metformin and inositol may also indirectly reduce androgen levels, although their specific effect on the clinical reduction of hirsutism and acne has not been shown.1 Anti-androgen agents such as spironolactone, cyproterone acetate and finasteride must be used with effective contraception given their teratogenicity; evidence also supports the reduction of hirsutism with the addition of an anti-androgen to CHCs.1
What are the fertility and pregnancy considerations for patients with PCOS?
If a patient intends to conceive, clinicians should communicate that irregular or prolonged (> 35 d) cycles may still be sporadically ovulatory.25 Conversely, contraception is needed if pregnancy is not desired. Time to pregnancy is longer on average; a large population-based study in Sweden observed that spontaneous conception took an average of 2 years longer among patients with PCOS.26 Ovulatory function and, thus, cycle regularity tend to improve as patients age, although all patients are subject to age-related fertility decline regardless of PCOS.27
In the population-based study from Sweden, the cumulative probability of childbirth after spontaneous conception was 55% among patients with PCOS, compared with 73.8% among women without PCOS.26 With assisted reproduction, the cumulative probability of childbirth was the same among both patients with PCOS (80%) and those without (78%).26 First-line options for management of return of ovulatory cycles that can be initiated by primary care physicians include weight loss of 5%–10% for patients with overweight or obesity, metformin, inositol or letrozole. 1 It is reasonable to trial these methods for 6–12 months in patients younger than 35 years. Metformin and inositol are safe in pregnancy; however, unless the patient has concurrent type 2 diabetes, no convincing evidence supports continuing these medications in pregnancy. Referral to a fertility specialist for ovulation induction with letrozole, gonadotropins or laparoscopic ovarian drilling (i.e., use of a monopolar needle to puncture the ovarian cortex) can be considered at any time.1
Pregnant patients with PCOS are at increased risk of miscarriage, gestational weight gain, gestational diabetes, hypertension, preeclampsia, intrauterine growth restriction, preterm delivery and cesarean delivery; some of the risks may be mitigated by maintenance of a normal BMI.1 Given the known contribution of PCOS to impaired glycemic status, screening for impaired fasting glucose or impaired glucose tolerance with a 75-g oral glucose tolerance test should be considered before conception.3 When not completed before conception, it should be performed at the first prenatal visit before 20 weeks’ gestation and again at 24–28 weeks’ gestation.1 Although the quality of evidence is low, an oral glucose tolerance test is the preferred method for identification of insulin resistance among patients with PCOS.1
What are the long-term health complications associated with PCOS?
Long-term complications such as hypertension, impaired glucose tolerance, type 2 diabetes, metabolic syndrome, non-alcoholic fatty liver disease, depression, anxiety, obstructive sleep apnea and cardiovascular disease (i.e., ischemic heart disease, myocardial infarction and cardiovascular mortality) have all been associated with PCOS.16 These conditions tend to present earlier among people with PCOS than age-matched controls.27 People with PCOS and a BMI greater than 25 are at higher risk of long-term health complications than patients with PCOS and a BMI of 25 or less. Ongoing care for patients can often be fragmented as the emphasis in PCOS can be overly focused on reproduction rather than long-term sequelae.28 Baseline and follow-up assessments, as outlined in Box 4, should be performed for all patients with PCOS.
Box 4: Baseline and annual health assessment in all patients with PCOS
Measurement of height, weight and body mass index
Measurement of blood pressure
Cardiovascular risk assessment including cigarette smoking, physical activity and family history of premature cardiovascular disease.
Assessment of lipid profile (cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol and triglycerides)
Assessment of glycemic status, ideally with oral glucose tolerance test
Assessment for obstructive sleep apnea symptoms (i.e., snoring with waking unrefreshed, daytime sleepiness or fatigue)
Screening for depression and anxiety
Screening for amenorrhea exceeding 90 d
Polycystic ovarian syndrome may be associated with hypertension. A recent meta-analysis showed that the risk of hypertension was increased only among patients of reproductive age (pooled RR 1.72, 95% confidence interval [CI] 1.43–2.07) but not among menopausal patients who had PCOS during their reproductive years (pooled RR 1.26, 95% CI 0.95–1.67).29 As such, patients with PCOS should have blood pressure measurements annually and at any time when fertility is desired since patients are at increased risk of hypertensive disorders in pregnancy.1
Data on cardiovascular risk outcomes show inconsistent findings, although this is likely owing to the low event rate of major adverse cardiovascular events among premenopausal women.28 Recently, several meta-analyses have suggested with very low to low certainty that females with PCOS have higher ORs or incidence rate ratios for composite cardiovascular disease, composite ischemic heart disease, myocardial infarction, stroke and cardiovascular mortality.1 Thus, monitoring of cardiovascular risk profiles, including lipid profiles, should be undertaken both at baseline and on an ongoing basis for all patients with PCOS.1
Polycystic ovarian syndrome is also related to hyperinsulinemia, impaired glucose intolerance and type 2 diabetes. 9,16,22 A meta-analysis of 41 studies indicated an increased risk of type 2 diabetes among patients with PCOS compared with those without PCOS (OR 2.87, 95% CI 1.37–6.01).1 Hyperinsulinemia is present in 75% of patients with PCOS and a BMI of 25 or less and 95% of patients with a BMI greater than 25.1
Polycystic ovarian syndrome is associated with a higher risk of obstructive sleep apnea, independent of BMI. In a recent meta-analysis of 8 studies, those with PCOS had a 10 times higher chance of obstructive sleep apnea than those without PCOS, with an odds ratio (OR) of 9.52 (95% CI 3.90–23.26).3 Patients with PCOS should be assessed for symptoms of obstructive sleep apnea, screened using appropriate tools (e.g., Berlin Questionnaire) and directed for a sleep study and treatment if obstructive sleep apnea is identified.3
Patients with PCOS also have a high prevalence of depression and anxiety. In a meta-analysis of 47 studies, depression was more likely among patients with PCOS than those without PCOS (OR 2.59, 95% CI 2.11–3.16).1 In a meta-analysis of 27 studies reporting on anxiety, patients with PCOS had a higher risk of anxiety than those without, with an OR of 2.68 (95% CI 2.08–3.44).1 Polycystic ovarian syndrome can have a negative impact on body image and self-esteem, and is also associated with a higher rate of disordered eating.1
Conclusion
Polycystic ovarian syndrome, a common endocrinological disorder among reproductive-aged females, presents with menstrual irregularities, hyperandrogenism and polycystic ovarian morphology. It is associated with important long-term health consequences such as hypertension, neoplastic risks, metabolic consequences, adverse cardiovascular outcomes, psychological impacts and adverse reproductive outcomes. Early diagnosis can allow for improvement in symptoms and mitigation of long-term health complications.
Footnotes
Competing interests: Mara Sobel reports an honorarium from Bayer. No other competing interests were declared.
This article has been peer reviewed.
Contributors: All of the authors contributed to the conception and design of the work, drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
Article extras
Article tools






Jump to section
- Article
- What is the pathophysiology of PCOS?
- What symptoms do patients with PCOS describe?
- How is PCOS diagnosed?
- How are the clinical manifestations of PCOS managed?
- What are the fertility and pregnancy considerations for patients with PCOS?
- What are the long-term health complications associated with PCOS?
- Conclusion
- Footnotes
- References
- Figures & Tables
- Related Content
- Responses
- Metrics
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

