


Abstract
Background: Food insecurity is a serious public health problem and is linked to the mental health of children and adolescents; however, its relationship with mental health service use is unknown. We sought to estimate the association between household food insecurity and contact with health services for mental or substance use disorders among children and adolescents in Ontario, Canada.
Methods: We used health administrative data, linked to 5 waves of the Canadian Community Health Survey, to identify children and adolescents (aged 1–17 yr) who had a household response to the Household Food Security Survey Module. We identified contacts with outpatient and acute care services for mental or substance use disorders in the year before survey completion using administrative data. We estimated prevalence ratios for the association between household food insecurity and use of mental health services, adjusting for several confounding factors.
Results: The sample included 32 321 children and adolescents, of whom 5216 (16.1%) were living in food-insecure households. Of the total sample, 9.0% had an outpatient contact and 0.6% had an acute care contact for a mental or substance use disorder. Children and adolescents in food-insecure households had a 55% higher prevalence of outpatient contacts (95% confidence interval [CI] 41%–70%), and a 74% higher prevalence of acute care contacts (95% CI 24%–145%) for a mental or substance use disorder, although contacts for substance use disorders were uncommon.
Interpretation: Children and adolescents living in a food-insecure household have greater use of health services for mental or substance use disorders than those living in households without food insecurity. Focused efforts to support food-insecure families could improve child and adolescent mental health and reduce strain on the mental health system.
Nearly 6 million people in Canada, including 1.4 million children younger than 18 years, faced food insecurity in 2021.1 Defined as the inability to acquire adequate food because of financial constraints, household food insecurity is a persistent problem across Canada, and families with children are at higher risk.1 However, the wider health implications of food insecurity for children in Canada are not well understood.
Mental and substance use disorders among children and adolescents is also a pressing public health concern.2 These conditions are the leading contributor to total burden of illness in high-income countries, and are responsible for the largest proportion of years lived with disability in this age group.2,3 Given the importance of early life adversity on the risk of mental and substance use disorders,4 the lasting effects of early life nutrition, 5 and the known relationship between food insecurity and adult mental health,6 it follows that household food insecurity may be an important social determinant of mental and substance use disorders among children and adolescents.
A recent systematic review concluded that even marginal levels of food insecurity had consequences for behavioural, emotional and academic outcomes throughout childhood and adolescence, including substance use disorders.7 However, previous studies that considered the relationship between mental health and food insecurity tended to focus on symptoms and behaviours, screening tools or self-and parent-reported diagnoses.7 The association between food insecurity and clinical diagnoses or use of mental health services has not been well studied, yet this could provide an indicator of the clinical importance of mental health outcomes, and could also inform the response of the mental health system to the problem of food insecurity. Moreover, Canadian evidence on the association between household food insecurity and mental and substance use disorders among children and adolescents remains limited.8–11
We sought to estimate the association between household food insecurity and contact with health services for mental and substance use disorders among children and adolescents younger than 18 years in Ontario, Canada.
Methods
Data sources
We accessed the data for this study through ICES, which is an independent research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. ICES collates data from the Ontario Health Insurance Plan (OHIP), which covers all medically necessary services for the eligible population of Ontario (> 96%). We used data from outpatient physician billings, community health centres, emergency department visits and hospital admissions, linked to sociodemographic and household food insecurity data from the Canadian Community Health Survey (CCHS). Maternal CCHS respondents were linked to their children using MOMBABY, an ICES-derived database that links inpatient records of people who deliver a child to their newborn’s birth records. We followed the Reporting of Studies Conducted using the Observational Routinely Collected Data (RECORD) checklist for observational studies using health administrative data (Appendix 1, Supplement 1–4, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.230332/tab-related-content).12
Study population
The CCHS is a cross-sectional population health survey of people in Canada aged 12 years and older. The study sample was based on 5 cycles of the CCHS (2005, 2007–2008, 2009–2010, 2011–2012, 2013–2014) that had been linked to health administrative data at ICES. We included children and adolescents (aged 1–17 yr) born in Ontario with a household response to the CCHS, identified in 3 ways, namely children and adolescents whose birthing parent completed the CCHS, identified using MOMBABY; adolescent respondents who completed the CCHS and had a record in MOMBABY; and siblings of adolescent CCHS respondents, identified by linking the birth parent of the adolescent respondents to other children and adolescents born in Ontario using MOMBABY. For birthing parents who completed the CCHS, we included only female respondents and the assumption was made that they identified as mothers.
We confirmed that children and adolescents were alive when the survey was completed and living with their birth parent or sibling using residential postal codes, obtained from the health administrative data. For children and adolescents identified across multiple waves of the CCHS (n = 157), we selected the first record. We excluded children and adolescents who were missing data on household food insecurity (< 1% of sample) or were ineligible for OHIP in the 12 months before the survey. We also excluded children and adolescents with a household CCHS interview date after Jan. 1, 2014, as the study cohort was derived as part of a larger study that required a prospective follow-up period.13,14
Exposure
Our exposure was household food insecurity, measured using the validated Household Food Security Survey Module.15 This module includes 18 items designed to assess the household’s financial ability to access adequate food over the previous 12 months. For adolescent CCHS respondents, an adult member of the household with knowledge of its economic circumstances completed the module, with the exception of the 2005 and 2007–2008 cycles, for which adolescents older than 16 years completed it. The experiences assessed included worrying about running out of food, inability to afford balanced meals, missing meals, and going days without eating because of financial constraints. We combined responses to determine household food insecurity status, categorized as food-secure, marginally food-insecure, moderately food-insecure or severely food-insecure (Appendix 1, Supplement 2).15 For our main analyses, we compared children with any level of household food insecurity with those who were food-secure, given evidence that even marginal food insecurity may have mental health and developmental effects.7 We used the 4-level variable for household food insecurity for descriptive and sensitivity analyses.
Outcomes
Our primary outcomes were any use of outpatient physician services and any use of acute care services (emergency department visits and hospital admissions) for a mental or substance use disorder in the 12 months before the CCHS interview date. For our secondary outcomes, we categorized diagnostic codes assigned to visits using a standardized definition of visits for mental disorders, which included psychotic disorders, mood or anxiety disorders, other selected disorders (e.g., eating disorders, personality disorders) and deliberate self-harm; visits for substance use disorders; and visits for neurodevelopmental disorders (e.g., autism, attention-deficit/hyperactivity disorder [ADHD], developmental delays) (Appendix 1, Supplement 3).16 Children and adolescents could contribute visits to more than 1 category.
Confounding factors
From the health administrative data, we obtained information on each child or adolescent’s age, sex at birth, rurality of residence, and maternal health service contacts for a mental or substance use disorder in the previous year. The CCHS provided additional sociodemographic data on factors known to be associated with food insecurity or use of health services for a mental or substance use disorder.1,17–19 These included household income (with the lowest 2 deciles categorized as low income), self-identified racial group (White, Black, East or Southeast Asian, West Asian or Arabic, South Asian, Latin American, other), single-parent household (yes, no, unknown) and the number of children in the household. We obtained information on maternal migrant status from the Immigration, Refugee and Citizenship Canada Permanent Resident database, classified as recent migrant (< 10 yr), settled migrant (10–19 yr) and general population. We also obtained data on survey wave and respondent type (self, mother, sibling) (Appendix 1, Supplement 4).
Statistical analysis
We used modified Poisson regression models with robust standard errors to estimate prevalence ratios for the association between household food insecurity and our primary and secondary outcomes.20 We accounted for clustering of siblings within households using a robust sandwich estimator for the covariance matrix. We first estimated unadjusted models, followed by a partially adjusted model with only key covariates (age, sex, rurality, low household income), given the low number of events for some outcomes. Where possible, we then estimated fully adjusted models, adding maternal migrant status, past-year maternal health service use for mental or substance use disorders, single-parent household, number of children in the household, survey wave and respondent type to the partially adjusted model.
In a sensitivity analysis, we used the same modelling approach to estimate the association between household food insecurity status (i.e., marginal, moderate, severe) and any service use for mental or substance use disorders (outpatient and acute care). We added a linear contrast to test for a gradient effect with increasing severity of food insecurity. We also conducted age-stratified analyses to explore effect modification for children in preschool and elementary school (aged 1–13 yr) versus high school (aged 14–17 yr).
We conducted all analyses at ICES using SAS version 9.4 (SAS Institute). The results are presented as prevalence ratios with 95% confidence intervals (CIs).
Ethics approval
The use of the data in this project is authorized under section 45 of Ontario’s Personal Health Information Protection Act (PHIPA) and does not require review by a research ethics board.
Results
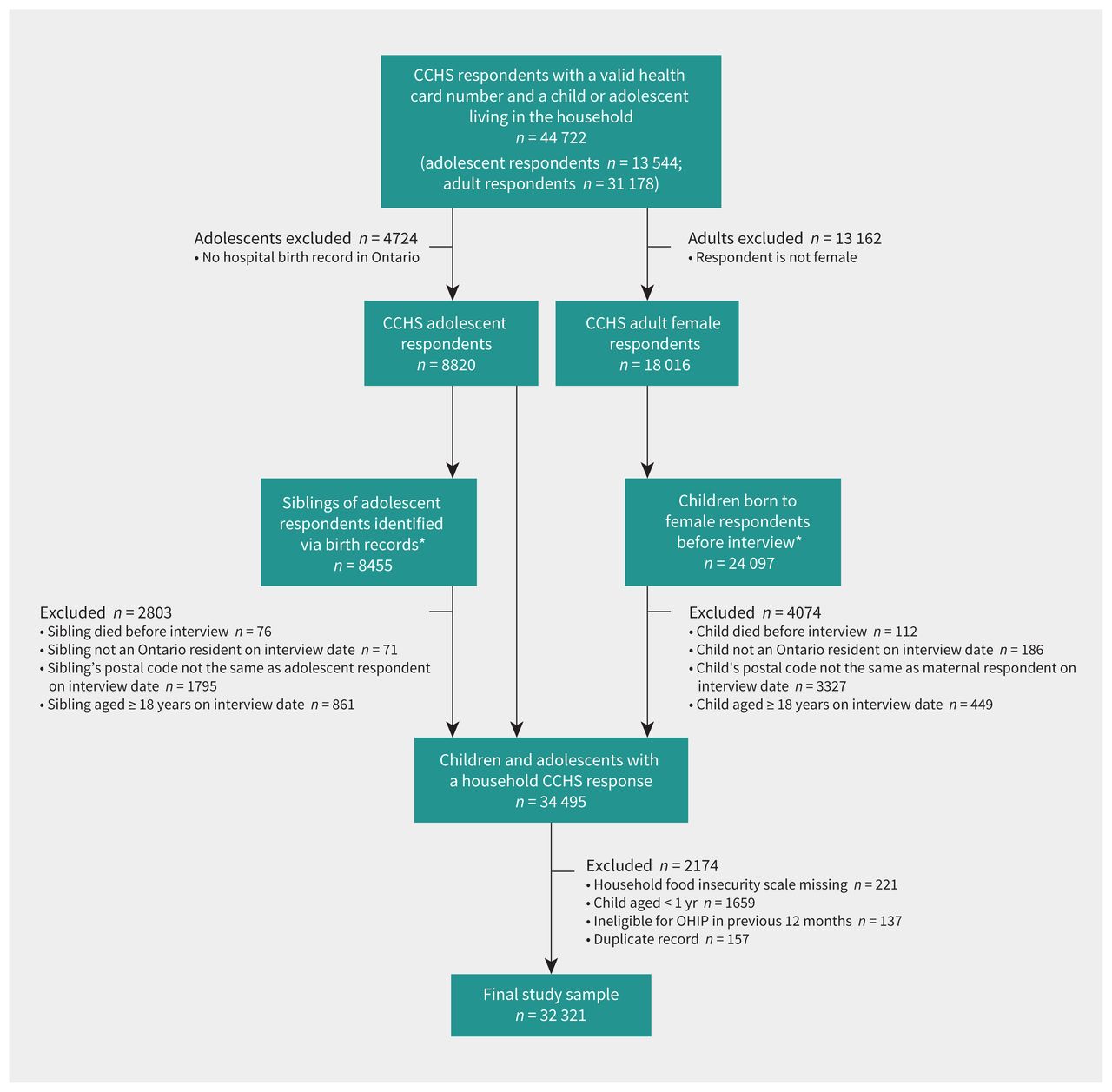
We analyzed data from a total sample of 32 321 children and adolescents, of whom 5216 (16.1%) were living in food-insecure households (1952 [6.0%] marginally food-insecure, 2348 [7.3%] moderately food-insecure, 916 [2.8%] severely food-insecure) (Figure 1). The sociodemographic characteristics of the sample, stratified by household food insecurity status, are presented in Table 1. Findings were consistent across the models (Appendix 1, Supplements 5–11), with some attenuation of effect with increasing levels of adjustment; therefore, our description of the findings focused on the partially adjusted models for consistency with models for which a fully adjusted estimate was not available.

Flow chart showing the derivation of the study sample using data from 5 waves of the Canadian Community Health Survey (CCHS), linked to health administrative data. *Sample derived through record linkage. Note: OHIP = Ontario Health Insurance Plan.
Sociodemographic characteristics of the children and adolescents included in the study sample, stratified by household food insecurity status
In the year before the survey, 2918 (9.0%) children and adolescents had an outpatient physician visit for a mental or substance use disorder, and 194 (0.6%) children and adolescents had an acute care contact, with evidence of increasing prevalence with increasing severity of food insecurity (Table 2). Food-insecure children and adolescents constituted 23.5% and 24.7% of those with outpatient or acute care visits for mental or substance use disorders in the previous year, respectively. The most common service contacts were for neurodevelopmental disorders (prevalence 4.1%–9.5%) and mood or anxiety disorders (prevalence 3.2%–5.0%), followed by social problems (prevalence 1.1%–1.4%) and other mental disorders (prevalence 1.2%–2.0%). Service contacts for psychotic disorders, substance use disorders and deliberate self-harm were uncommon.
Frequency of outpatient visits, acute care visits (emergency department visits and hospital admissions) and visit diagnoses, by household food insecurity status among children and adolescents in Ontario, Canada
Children and adolescents from food-insecure households had a 55% higher prevalence of outpatient visits for mental or substance use disorders in the previous year, relative to those from food-secure households (prevalence ratio 1.55, 95% CI 1.41–1.70). Similarly, children and adolescents from food-insecure households had a 74% higher prevalence of acute care visits in the previous year, relative to those from food-secure households (prevalence ratio 1.74, 95% CI 1.24–2.45). The findings were consistent in our secondary analyses and showed an association between household food insecurity and visits for mental disorders (prevalence ratio 1.43, 95% CI 1.25–1.64), substance use disorders (prevalence ratio 2.26, 95% CI 1.18–4.33) and neurodevelopmental disorders (prevalence ratio 1.71, 95% CI 1.50–1.95) (Table 3 and Appendix 1, Supplements 5–9).
Association between any household food insecurity and use of health services for a mental or substance use disorder, relative to food-secure households, among children and adolescents in Ontario, Canada
The results of sensitivity analyses using household food insecurity status largely aligned with those of the main analyses (Table 4 and Appendix 1, Supplement 10). We found evidence of a gradient effect, with prevalence increasing with increasing severity of food insecurity (test for trend prevalence ratio 1.25, 95% CI 1.21–1.31). The age-stratified analysis showed slightly higher effect estimates for adolescents in high school (aged 14–17 yr; prevalence ratio 1.69, 95% CI 1.45–1.97), relative to children in preschool and elementary school (age 1–13 yr; prevalence ratio 1.48, 95% CI 1.32–1.66); however, the test for effect modification was not statistically significant (p = 0.06) (Appendix 1, Supplement 11).
Association between household food insecurity status and use of any health services for a mental or substance use disorder among children and adolescents in Ontario, Canada (sensitivity analysis)
Interpretation
Children and adolescents living in food-insecure households in Ontario had a higher prevalence of past-year health service contacts for mental or substance use disorders, and this was not fully accounted for by key confounding factors, such as low household income, single-parent family, number of children in the household or maternal mental or substance use disorders. 1,17–19 We also found some evidence that contact with services for a mental or substance use disorder increased with increasing severity of household food insecurity.
Our findings align with previous evidence showing a higher prevalence of psychiatric symptoms and self-reported diagnoses, as well as poorer psychosocial functioning, among children and adolescents experiencing food insecurity in Canada.8–11 Our findings further suggest that these mental health outcomes are linked to increased health service use for mental and substance use disorders and contribute to higher health system costs.21 Adults experiencing food insecurity in Ontario also have higher health service use for mental and substance use disorders, as well as higher health system costs.22,23
The disproportionately higher use of health services for mental and substance use disorders among children and adolescents in food-insecure households was predominantly driven by visits for neurodevelopmental and mood and anxiety disorders. This is consistent with previous research showing that children and adolescents experiencing food insecurity are more likely to have symptoms of depression and anxiety, a worsening of ADHD symptoms and other behavioural issues.7–10,17,24–26 Food insecurity has also been associated with suicidal ideation and attempts among adolescents,8,9,27 but we found no indication of a higher prevalence of acute care visits for self-harm, although these were uncommon in our sample. The coexistence of household food insecurity and service use for mental and substance use disorders is problematic, given that both of these conditions have each been found to have negative consequences for social, educational and developmental outcomes among children and adolescents.7,28
Children and adolescents from marginalized groups have been shown to have poorer access to mental health care;29 therefore, we have likely underestimated the magnitude of association between household food insecurity and health service use for mental and substance use disorders. Food insecurity is a marker for more widespread and pervasive material deprivation; 1 although it is plausible that household food insecurity may be a direct cause of mental and substance use disorders,30 it is likely to be a marker of risk for a myriad of interconnected socioeconomic factors that contribute to mental and substance use disorders among children and adolescents. Furthermore, mental and substance use disorders may be poorly managed for children and adolescents in food-insecure households, irrespective of the causal mechanism. Future research using complex modelling approaches could better estimate the relative contributions of these social determinants.
Limitations
Our findings are limited to Ontario and are not necessarily generalizable to First Nations groups and people living in remote areas, where food insecurity is particularly prevalent.1 Furthermore, the original survey sampling was not retained for the sample we analyzed and, therefore, survey weights could not be applied to ensure a representative sample (Appendix 1, Supplement 12 provides a comparison of our sample with the characteristics of Ontario households from the 2011 Census; we may have under-represented children from some racial minority groups, recent migrants and those from single-child families). The data used in this study are nearly a decade old, as this was the last available wave of CCHS data linked to the ICES data holdings. The most recent data on food insecurity in Canada suggest that the prevalence of household food insecurity has increased in the intervening years, particularly during the COVID-19 pandemic.31 Other provinces have a higher prevalence of food insecurity than Ontario.1 Assuming that the associations we observed have continued over time and are generalizable across provinces, we would expect more recent pan-Canadian data to show an even greater proportion of children and adolescents from food-insecure families seeking treatment for mental and substance use disorders.
Given the cross-sectional design of our study and the 12-month assessment of exposure and outcome variables, we are unable to establish the temporal relationship between household food insecurity, potential confounders and mental health and substance use problems among children and adolescents. It is possible that a child or adolescent’s mental or substance use disorder may contribute to household food insecurity (e.g., out-of-pocket costs for therapy or medication), although previous Canadian research found that people from food-insecure households are more often nonadherent to medication.32
Child and adolescent mental health services in Ontario are delivered across several sectors;16 missing information on use of mental health services outside of the public-payer health care sector — including community-based mental health programs or school-based psychologists, as well as private-payer services, which are likely used more frequently by food-secure children — may have affected our results. Because the study sample was derived from birth record linkages, father-only families are likely under-represented and information on paternal mental and substance use disorders is missing. Finally, information on the duration of household food insecurity was not available to allow us to explore the effects of cumulative exposure.
Conclusion
Our study adds to a growing body of evidence that suggests that household food insecurity is linked to adverse mental health outcomes among children and adolescents. Household food insecurity represents a modifiable marker of risk for mental and substance use disorders, with evidence of effective public policy interventions. Focused efforts to support food-insecure families should be explored as a target for public mental health efforts to improve child and adolescent mental health and reduce the strain on the mental health system.
Footnotes
Competing interests: Kelly Anderson reports funding from the Department of Psychiatry Seed Fund Competition, the Petro Canada Young Innovator Award and the Canadian Institutes of Health Research. Kristin Clemens reports honoraria from the CPD Network and the Canadian Medical and Surgical Knowledge Translation Research Group. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Kelly Anderson, Kristin Clemens, Britney Le and Salimah Shariff contributed to conception and design of the study. All of the authors contributed to data analysis and interpretation. Kelly Anderson drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study received funding from the Children’s Health Research Institute (London, Ont.). Kelly Anderson is supported by a Tier 2 Canada Research Chair in Public Mental Health Research. The funders did not have a role in the research.
Data sharing: The data set from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (e.g., health care organizations and government) prohibit ICES from making the data set publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at www.ices.on.ca/DAS (email: das{at}ices.on.ca). The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification. The ICES analysts (Britney Le, Lixia Zhang) had full access to the study database.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This study used data adapted from the Statistics Canada Postal Code Conversion File, which is based on data licensed from Canada Post Corporation and/or data adapted from the Ontario MOH Postal Code Conversion File, which contains data copied under license from Canada Post Corporation and Statistics Canada. Parts of this material are based on data and information compiled and provided by the Ontario MOH, the Canadian Institute of Health Information (CIHI) and Immigration, Refugee, and Citizenship Canada (IRCC). This study also used data adapted from Statistics Canada (Canadian Community Health Survey 2005, 2007–2008, 2009–2010, 2011–2012 and 2013–2014). This does not constitute an endorsement by Statistics Canada of this product. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
- Accepted June 13, 2023.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

