


- © 2007 Canadian Medical Association or its licensors
Abstract
Cardiovascular disease (CVD) is the leading cause of mortality in women. In fact, CVD is responsible for a third of all deaths of women worldwide and half of all deaths of women over 50 years of age in developing countries. The prevalence of CVD risk factor precursors is increasing in children. Retrospective analyses suggest that there are some clinically relevant differences between women and men in terms of prevalence, presentation, management and outcomes of the disease, but little is known about why CVD affects women and men differently. For instance, women with diabetes have a significantly higher CVD mortality rate than men with diabetes. Similarly, women with atrial fibrillation are at greater risk of stroke than men with atrial fibrillation. Historically, women have been underrepresented in clinical trials. The lack of good trial evidence concerning sex-specific outcomes has led to assumptions about CVD treatment in women, which in turn may have resulted in inadequate diagnoses and suboptimal management, greatly affecting outcomes. This knowledge gap may also explain why cardiovascular health in women is not improving as fast as that of men. Over the last decades, mortality rates in men have steadily declined, while those in women remained stable. It is also becoming increasingly evident that gender differences in cultural, behavioural, psychosocial and socioeconomic status are responsible, to various degrees, for the observed differences between women and men. However, the interaction between sex-and gender-related factors and CVD outcomes in women remains largely unknown.
Burden of cardiovascular disease in women and men
Doreen Rabi and Jafna Cox
Although cardiovascular disease (CVD) is common, significant sex-related differences in its epidemiology have only recently been appreciated. The objective of this section is to demonstrate that there are sex-specific differences in the prevalence, complications and burden of CVD in terms of mortality, hospital admissions and quality of life.
Search strategy
A MEDLINE search was conducted using the MeSH terms “cardiovascular disease” OR “atrial fibrillation” OR “congestive heart failure.” A second search used the terms “prevalence” OR “incidence” OR “mortality” and the final search combined the results of the first 2 searches and added the terms “gender” OR “sex.” Articles identified in this manner were retrieved and their reference lists searched for additional relevant articles. The search was limited to English-language publications, but no other restrictions were applied. Other data sources included Web sites of the World Health Organization, the Canadian Institute for Health Information and the National Centre for Health Statistics. Thirty-three original studies were reviewed. Studies were included if they were cohort studies, case–control studies or nested cohort studies that examined the incidence, prevalence or mortality of CVD, congestive heart failure or atrial fibrillation. The studies had to include data on both men and women.
Cardiovascular disease
Prevalence
CVD is ubiquitous. Determining the extent of the burden this disease places on society is difficult as most databases and studies base the presence of CVD on presentation with an acute event, making the prevalence of asymptomatic disease difficult to establish. Public health surveys have been used to determine the prevalence of CVD in the ambulatory population. North American surveys indicate that CVD is diagnosed more frequently in men, with 5.4% of Canadian men (compared with 4.6% of women)1 and 8.4% of US men (compared with 5.6% of women)2 reporting a prior diagnosis of CVD.
Trends in CVD vary considerably from region to region.3 In North America, Europe, Australasia and middle-income developing countries, men are reported to have a higher prevalence of CVD compared with women (Table 1).4 However, the proportion of women presenting with clinically and angiographically significant disease has increased over the last 20 years. Overall, the incidence of CVD, and of coronary artery disease (CAD) in particular, has been declining in men but has remained stable in women.5
Table 1.
Mortality
CVD remains a leading cause of mortality throughout the world, affecting both women and men.6 Trends in CVD mortality, like trends in prevalence, display regional variations (Fig. 1).7 Although the age-standardized mortality rates have been declining over the past 3 decades in Western Europe and North America, they have risen markedly in middle-income developing countries (Eastern Europe and China). Levi and colleagues8 demonstrated that these trends are consistent for both men and women (Fig. 2).

Fig. 1: Changes in rates of death from cardiovascular disease among men and women aged 35–74 years between 1990 and 2000 in selected countries. Reproduced with permission from the World Health Organization.7
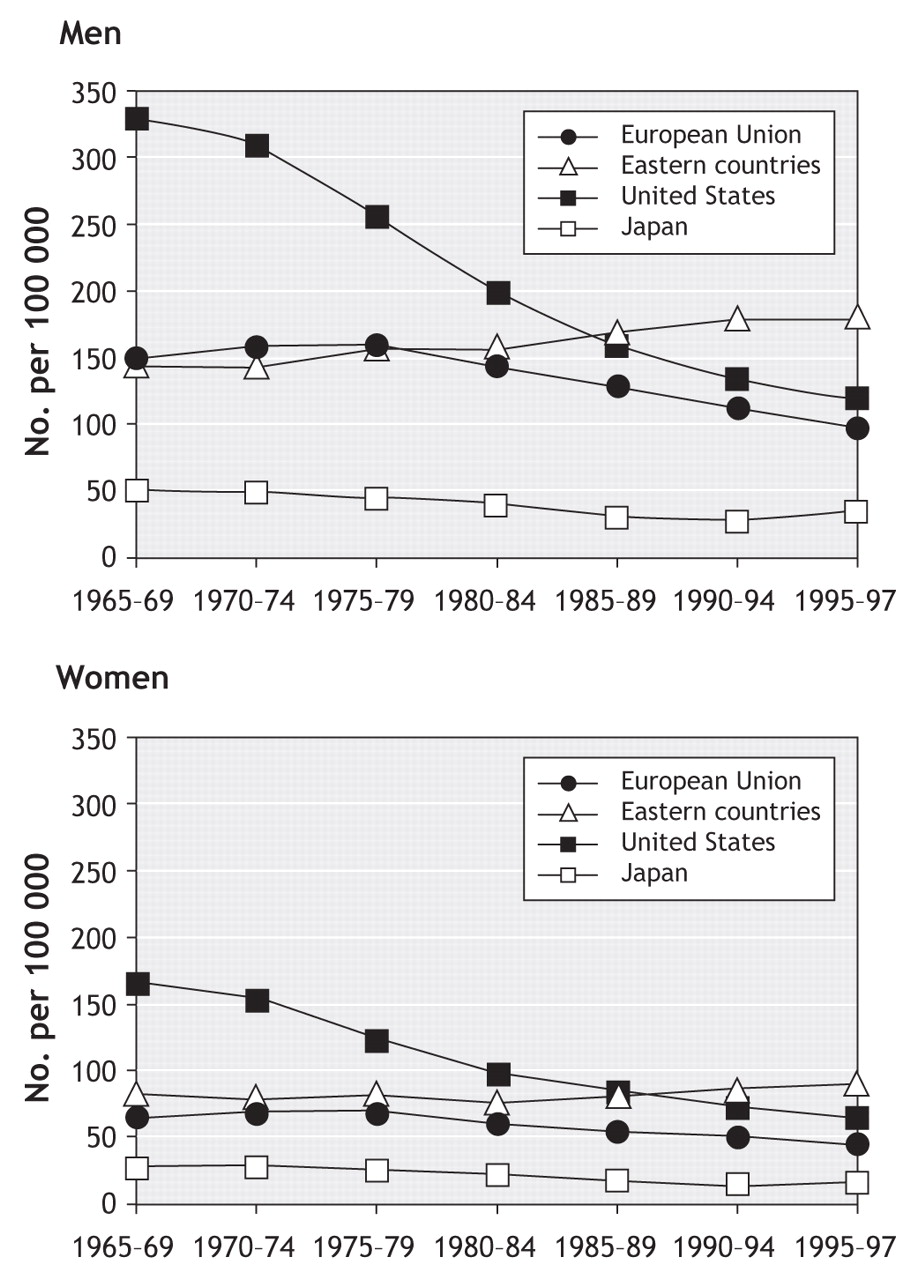
Fig. 2: Trends in age-standardized (world population) cardiovascular disease mortality among men and women in the European Union, Eastern Europe (Bulgaria, Czech Republic, Hungary, Poland, Romania and Slovakia), the United States and Japan from 1965 to 1972. Reproduced with permission from BMJ Publishing Group (Heart 2002;88:119-24).8
Historically, men have had higher cardiovascular-related mortality rates than women. This finding is consistent across several countries. According to Manuel and colleagues,9 in 1999, Canadian men had an age-standardized CVD mortality rate of 288 per 100 000, while the rate for women was 175 per 100 000. Sex-specific, age-standardized CVD mortality rates were very similar in the United States in 2003: 307 per 100 000 for men and 158 per 100 000 for women.2 At the international level, CVD mortality rates are consistently higher in men (Table 2).6
Table 2.
Hospital admissions
CVD is the leading cause of admission to hospital in North America for both men and women. In 2000, CVD accounted for 18% of all hospital admissions in Canada. Women experience longer stays in hospital related to CVD and suffer greater disability. The National Population Health Survey1 revealed that among respondents reporting a diagnosis of heart disease, women consistently reported higher levels of pain, discomfort, activity restriction and disability secondary to their heart disease than men.
Coronary artery disease
Men continue to have higher rates of mortality related to acute myocardial infarction (AMI) and CAD than women. In Canada in 1999, the age-standardized CAD mortality rate for men was 188 per 100 000 compared with 97 per 100 000 for women.9 A similar sex difference was noted in the United States in 2003 when the CAD mortality rate per 100 000 was 187 for men and 77 for women.2 This difference appears to be consistent across international borders (Table 2).6 However, younger women with AMI have higher rates of mortality than men of the same age.10–12
Heart failure
Prevalence
Heart failure, a recognized complication of CAD and AMI, has become more prevalent over the past several years. Recent data from the Framingham study suggest that the lifetime risk of developing heart failure is about 20% for both men and women.13 Approximately 2% of people living in the Americas have a diagnosis of heart failure. The prevalence is similar in Europe, where it is estimated to be between 1.8% (95% confidence interval [CI] 1.4–2.3)14 and 3.9% (95% CI 3.0–4.7),15 and it is as high as 6.3% (95% CI 5.0–7.7) in Australia.16 The risk of left-ventricular systolic dysfunction increases steadily with age in both men and women. After the age of 75 years, the prevalence of heart failure secondary to systolic dysfunction is estimated to be 8.4%.17,18
In Canada, as elsewhere, most patients with heart failure are 65 years of age and older, with women comprising 51% of all new cases.19 As with ischemic heart disease, female patients with heart failure are older than males and more likely to be hypertensive and diabetic, but they tend to have better preserved systolic function, a lower prevalence of ischemic etiology and are less likely to have a history of prior AMI.20,21
Mortality
Once heart failure is present, the median survival time is 1.7 years for men and 3.2 years for women.13 Mortality following a diagnosis of heart failure remains significant. The 5-year mortality rate is approximately 50% for both women and men. Although mortality associated with heart failure has declined significantly over the past 20 years in men (28%–52%), the decrease has not been as significant in women (6%–33%).22
Hospital admissions
Heart failure is a leading cause of hospital admission throughout the world, and women account for about 50% of these admissions. In North America, admissions to hospital with a primary diagnosis of heart failure have increased by 34% since 1990, but this increase is more notable in women (39%) than men (29%). In fact, a review of the American National Hospital Discharge Survey23 noted that age-adjusted heart failure admission rates have been constant since 1991 for men, but have continued to increase for women (19%) (Fig. 3), suggesting that the increase in hospital admissions in recent years is largely the result of more women presenting with clinically significant disease. Once discharged from hospital, men and women appear to have similar rates of readmission (hazard ratio [HR] 0.89; 95% CI 0.71–1.11).21 Sex differences in length of hospital stays have also been noted, with women having significantly longer hospital stays than men.24

Fig. 3: American National Hospital Discharge Survey data on annual hospital admissions because of heart failure among adults 35 years and older, 1990–2000. Reproduced with permission from Elsevier (Am Heart J 2004;147:74-8).23
Atrial fibrillation
Prevalence
Atrial fibrillation is the most common cardiac arrhythmia and is an established risk factor for stroke and premature death. North American and European studies indicate that about 0.95%–1.1% of the population experiences atrial fibrillation.25–27 The Framingham study demonstrated that men were 1.5 times more likely to develop atrial fibrillation than women,28 but because the number of women older than 75 years is almost twice that of men, the absolute numbers of those with atrial fibrillation are roughly equal.26 Incidence increases with age; the prevalence of atrial fibrillation at age 55 is 0.1% and increases to 9.0% in those over 80 years of age.26,29 This age-related increase in prevalence is most striking in men (Table 3).30
Table 3.
Mortality
Mortality rates are significantly higher in both women and men with atrial fibrillation. In longitudinal studies, mortality rates were approximately 25% higher than age-and sex-matched controls.31,32 In the United States, in-hospital mortality rate following admission for atrial fibrillation is estimated at 0.8%. Men have a modestly higher (but statistically significant) risk of in-hospital mortality. Using administrative data (National Hospital Discharge Survey), Kairallah and colleagues33 demonstrated that male sex was an independent predictor of in-hospital mortality (odds ratio [OR] 1.10; 95% CI 1.06–1.14). However, analysis of administrative data from Scotland suggests that 1-year mortality may be higher in women; Stewart and colleagues34 found the 1-year case fatality rate in men to be 11.9% v. 16.2% in women. The distribution of ages in this cohort is not known; the higher mortality rate seen in women may reflect a greater number of very elderly women diagnosed with atrial fibrillation. Wattigney and colleagues35 have demonstrated in a US cohort that mortality remains higher among men after age standardization.
Hospital admission and stroke
Reflecting the sex differences in prevalence, admissions to hospital for atrial fibrillation are also more common in men at every age (Table 4).36 Among patients with atrial fibrillation, women seem to be at greater risk of stroke than men. In a cohort of US Medicaid patients, Wolf and colleagues31 found that, after controlling for other established risk factors, women with atrial fibrillation had a 22%–25% greater risk of stroke than women without atrial fibrillation (Table 5). In contrast, the increased risk of stroke in men with atrial fibrillation was completely attenuated by controlling for other stroke risk factors.31 Women have also been found to have higher readmission rates following stroke.36
Table 4.
Table 5.
Health-related quality of life
Although men are more likely to die from CAD, women are more likely to live with CAD-related disability. In North American cohort studies, women with a history of CAD, heart failure or atrial fibrillation consistently report lower health-related quality of life and greater disability related to their heart disease than men. Women are also less likely to return to work following admission to hospital for complications related to CVD.37
Summary
• CVD is prevalent among both women and men.
• Women have a lower CVD mortality rate than men.
• CAD and atrial fibrillation are more prevalent among men than among women.
• Women appear to have a relatively higher risk of atrial fibrillation-related stroke than men.
• Clinically significant heart failure is on the rise in women.
• Women are more likely to live with more CVD-related disabilities and have a lower health-related quality of life.
Knowledge gap
• Why are CVD incidence and mortality rates decreasing among men but stable among women?
Cardiovascular risk factors in girls and boys
Jennifer McGrath, Tracie Barnett, MarieLambert, Jennifer O'Loughlin, GillesParadis, Arsham Alamian and Teresa Ho
Although most cardiovascular events occur in adulthood, the precursors of CVD manifest during childhood and adolescence.38,39 CVD is partly attributable to modifiable lifestyle behaviours, and childhood is a critical developmental period when these habits are established.40 Further, risk factors such as smoking, sedentary behaviour and poor diet in children and adolescents persist through young adulthood and are important predictors of subsequent risk of CVD.41–44 Consequently, it is essential to promote cardiovascular health and direct primary prevention efforts toward children and adolescents to disrupt the progression of CVD risk factors and thereby offset both the risk of CVD in adulthood and the unprecedented potential burden on health care systems.
Search strategy
Studies included in this qualitative review of childhood cardiovascular risk factors were identified through the use of widely available computer databases (Ovid MEDLINE, Ovid EMBASE, PubMed, PsycInfo, the Cochrane Library). Boolean searches were carried out by combining the keyword (“boy” OR “girl” OR “child” OR “pediatric” OR “adolescent” OR “young adult”) with each of the following keyword combinations using the AND operator: (“atherosclerosis” OR “cardiovascular” OR “coronary” OR “heart”), (“obesity” OR “overweight”), (“lipids” OR “lipoprotein”), (“hypertension” OR “blood pressure” OR “systolic” OR “diastolic”), (“cigarettes” OR “smoking” OR “tobacco”), (“diet” OR “nutrition”), (“exercise” OR “physical activity” OR “sedentary”), (“clustering” OR “behavior” OR “lifestyle”). Web sites of several well-known organizations, such as the World Health Organization, Centers for Disease Control and Prevention (CDC), Heart and Stroke Foundation of Canada and the American Heart Association, were reviewed for additional information and current recommendations. Finally, to obtain information from national and international statistical databases as well other “grey literature” and nonconventional documents, government Web sites (e.g., Statistics Canada, Health Canada, CDC) were examined. To reduce the copious amount of information this search strategy produced, the review emphasized children or adolescent populations; large studies with representative samples; longitudinal studies; and recent publications that reported sex-or gender-specific findings.
Overweight and obesity
Overweight and obesity are the most frequent nutritional disorders in industrialized countries in children as well as in adults; the prevalence of obesity has increased almost 3-fold over the past 2 decades.45,46 Although it is generally thought that girls are more likely to be overweight than boys, there are no differences in prevalence between girls and boys.
In a recent report based on heights and weights measured in the National Longitudinal Survey of Children and Youth47 and using Cole and colleagues'48 age-and sex-specific body mass index (BMI) threshold values for overweight and obesity, Shields46 estimated that the prevalence of overweight and obesity of Canadian boys and girls aged 2–17 years was 27% and 25%, respectively; the corresponding figures for obesity only were 9% and 7%, respectively. Although the overall prevalence of overweight and obesity was similar for boys and girls, trends varied for different age groups. The percentage of overweight and obese children 2–5 years old remained unchanged (21%) between 1978–1979 and 2004. However, the prevalence of overweight and obesity doubled among those 6–11 years (from 13% to 26%) and those 12–17 years (from 14% to 29%), and the prevalence of obesity tripled among those 12–17 years (from 3% to 9%). Secular trends in body mass of Canadian children are shown in Fig. 4.49 Part of these sex-based differences may be attenuated by the fact that age-and sex-specific thresholds are used to define overweight and obesity.
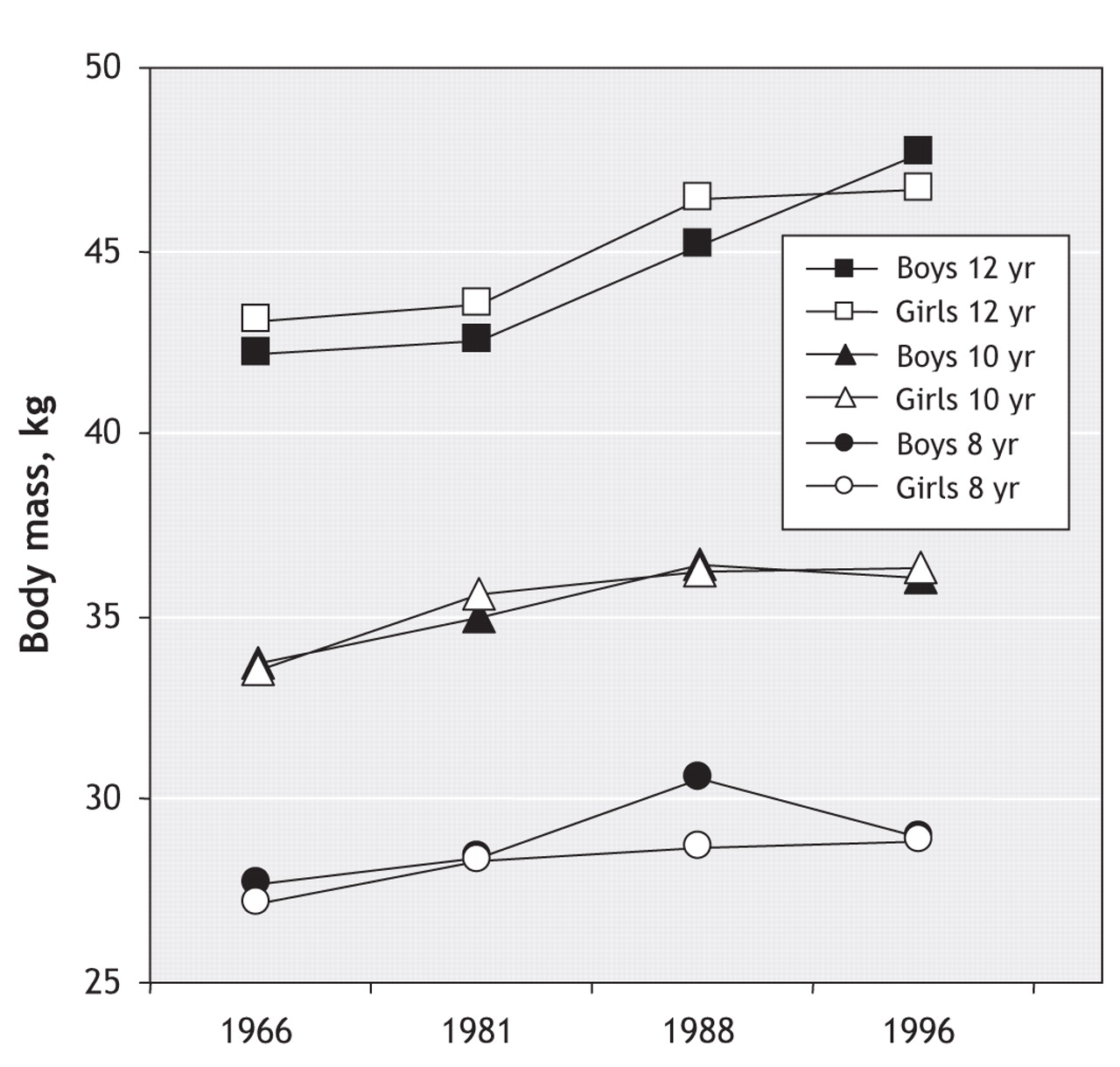
Fig. 4: Trends in body mass of Canadian boys and girls. Source: Adapted from Tremblay and Willms.49
In the United States, using height and weight measurements obtained in 1999–2000 as part of the National Health and Nutrition Examination Survey (NHANES) and the 2000 CDC growth chart reference values, Ogden and colleagues45 reported that the prevalence of overweight and obesity was 20.5%, 26.2% and 26.5% among non-Hispanic white youth aged 2–5, 6–11 and 12–19 years, respectively. The corresponding figures for obesity only were 10.1%, 11.8% and 12.7%. The prevalence of obesity was not significantly different for boys and girls.
Longitudinal studies have shown that measures of BMI taken during childhood and adolescence predict adult values. In the Bogalusa Heart Study,50 childhood and adult BMI were moderately correlated (Spearman's rank correlation coefficient 0.58), and this relation did not vary significantly with age, ethnic origin or sex. Similar results were observed in the Child and Adolescent Trial for Cardiovascular Health where the Kendall index of concordance for BMI was 0.86 over a follow-up period of 6 years and tracking was similar for both sexes.51
Summary
• The prevalence of obesity has increased almost 3-fold over the past 2 decades.
• There are no significant differences between girls and boys in the prevalence of overweight and obesity.
• A large proportion of obese adolescents will become obese adults.
Knowledge gap
• Additional research is needed on factors that contribute to the onset of overweight or obesity in childhood and adolescence and factors that contribute to its persistence into adulthood.
• The basic biologic characteristics of appetite, weight control, genetic susceptibility and environmental triggers remain elusive.
• We do not know specific prevention or treatment strategies that have sustained benefits in a broad spectrum of individuals.
Lipids and insulin resistance
Overweight and obesity are associated with significant health problems in the pediatric population and are important early risk factors for much of the adult morbidity and mortality associated with type 2 diabetes mellitus and CVD.
A large number of studies have consistently shown associations among childhood obesity, dyslipidemia, hyperinsulinemia and high blood pressure.52–54 The clustering of these CVD risk factors defines the metabolic syndrome called insulin resistance syndrome (IRS). The likelihood of IRS is the same for girls and boys. In the 1999 Quebec Child and Adolescent Health and Social Survey (QCAHS), a representative cross-sectional survey of Quebec youth, the overall prevalence of IRS was 11.5% in youth aged 9, 13 and 16 years.55 This is the only report on the prevalence of IRS in a provincially representative sample of youth in Canada. Findings from the third NHANES survey show a prevalence of IRS of 9.2% (95% CI 7.8–10.6) in US youth aged 12–19 years.56 Prevalence was comparable for girls (8.9%; 95% CI 7.1–10.7) and boys (9.5%; 95% CI 7.5–11.5) and for older (8.3%; 95% CI 6.5–10.1) and younger (10.3%; 95% CI 8.3–12.3) adolescents. The ethnic distribution was similar to that in adults: Mexican Americans (12.9%; 95% CI 10.4–15.4) and non-Hispanic white people (10.9%; 95% CI 8.4–13.4) had a greater prevalence of IRS compared with non-Hispanic black people (2.5%; 95% CI 1.3–3.7). Nearly a third (31.2%; 95% CI 28.3–34.1) of overweight or obese adolescents had IRS.
Given the link between excess weight and dyslipidemia, the increase in overweight and obesity among youth in North America is expected to affect trends in lipid and glucose levels adversely. However, comparing data from 2 NHANES surveys of US youth aged 4–17 years in 1988–1994 and 1999–2000, Ford and colleagues57 found that the mean concentrations of total cholesterol, high-density lipoprotein (HDL) cholesterol and low-density lipoprotein (LDL) cholesterol were almost the same in the 2 groups. However, in 1999–2000, mean triglyceride concentration was almost 10% lower than in 1988–1994 and mean glucose concentration decreased by 3%. These inconsistent trends in CVD risk factors, especially in HDL cholesterol and triglyceride levels, are difficult to explain. Changes in mean levels may not be sensitive enough to detect variations occurring at the extremities of the distributions; it would have been interesting to compare selected percentiles in the 2 surveys.
Although longitudinal data for plasma lipid levels in Canadian youth are not available, mean concentrations of plasma lipids in the 1999 QCAHS and in the 1999–2000 NHANES were similar.55,57 Body composition and fat distribution are different between boys and girls and across ages, and these differences may influence the relation between fatness and lipids.
Summary
• There are no significant differences between girls and boys in prevalence of IRS.
• There are no significant differences in the trends in lipid and glucose profiles of girls and boys over the last decade.
Knowledge gap
• Little is known about the natural history of the metabolic consequences of excess adiposity in childhood and adolescence.
• Surveillance of trends in obesity and the potential effects on CVD risk factors is needed.
• Better understanding of the relative importance of genetic, biologic, environmental and psychosocial determinants of metabolic abnormalities associated with excess fat is required.
Blood pressure
Knowledge of blood pressure distributions in youth is important: both systolic and diastolic pressure persist from childhood to adulthood42,58,59 and the current youth obesity epidemic has important effects on blood pressure distribution in this segment of the population.60
There are few data on blood pressure distribution and the prevalence of elevated blood pressure in Canadian children. The 1999 QCAHS reported important increases in mean systolic blood pressure and in height-specific systolic blood pressure percentile values compared with reference values from the National High Blood Pressure Education Program Working Group on Hypertension Control in Children and Adolescents61 for both boys and girls in all age groups.52 The proportion of children aged 9, 13, and 16 years with high-normal or elevated systolic pressure was 12%, 22% and 30%, respectively, for boys and 14%, 19% and 17% for girls. Elevated systolic pressure occurred in almost twice as many 16-year-old boys as girls. The mean systolic pressure of 13- and 16-year-old boys was 2 mm Hg (p = 0.004) and 10 mm Hg (p < 0.0001) higher, respectively, than that of girls. Less than 1% of youth had elevated or borderline diastolic blood pressure, and this did not differ between sexes. These findings were recently confirmed in a longitudinal study of Canadian adolescents. The likelihood of high systolic blood pressure values among boys compared with girls was 1.29 (95% CI 0.77–2.16) in grade 7, 1.98 (95% CI 1.35–2.93) in grade 9, and 2.74 (95% CI 1.52–4.94) in grade 11.62
A similar trend in high blood pressure has been observed in US children (Fig. 5).63 In age-matched boys and girls,64 cross-sectional analyses of the baseline data from the National Heart, Lung, and Blood Institute Growth and Health Study showed significantly higher systolic (105 v. 100 mm Hg) and diastolic (71 v. 65 mm Hg) blood pressure levels among overweight white girls aged 9 years than among those who were not overweight.65

Fig. 5: Trends in systolic and diastolic blood pressure among children and adolescents in the United States. Source: Adapted from Muntner et al.63
Limited data are available from representative samples of children from other parts of the world. Comparisons are further complicated by variations in sampling design and blood pressure measurement. For example, a recent survey of 809 boys and 842 girls aged 7–14 years from Belgrade, Serbia and Montenegro revealed average blood pressures of 113/70 mm Hg in boys and 115/71 mm Hg in girls. High systolic pressure was present in 5% of boys and girls, and high diastolic pressure was found in 6% of boys and 5% of girls.66 Conversely, a study of over 1200 children aged 6–11 years in Milan reported a significantly higher prevalence of elevated blood pressure in girls (5%) than in boys (3%).58 Sex differences in blood pressure may be due to differences in BMI between boys and girls at any given age, differences in activity levels and differences in pubertal stage at any given age.
Summary
• Elevated blood pressure persists from childhood to adulthood.
• Elevated blood pressure is prevalent in both girls and boys.
• Boys have higher systolic blood pressure than girls.
Knowledge gap
• Criterion-related reference values are necessary to clarify the significance of blood pressure levels in youth.
• More information is needed on blood pressure distribution and the prevalence of elevated blood pressure in groups of Canadian girls and boys.
• Sex differences in blood pressure require explanation at biologic, environmental and behavioural levels.
Smoking
Although data from the Global Youth Tobacco Survey67 and the National Tobacco Information Online System68 suggest that, in many developing countries, proportionately more boys than girls smoke, there have been few notable differences in the prevalence of smoking by boys and girls in developed countries over the last decade.69 Recent data for Canadian youth70,71 concur (Fig. 6).72 In Canada, 25% of girls 15–17 years old smoke compared with 19% of same-age boys, but by age 19 the prevalence is equal (31%).73 However, there appear to be sex differences in the number of cigarettes smoked per day, at least among young daily smokers. In 2002, Canadian boys in grades 5–9 smoked 8.8 cigarettes a day on average, compared with 7.3 cigarettes among girls.70 There are currently no nationally representative data comparing the incidence of smoking initiation by sex, although 1 prospective Canadian study suggests that boys are more likely than girls to escalate cigarette consumption rapidly after initiation.74 Although smoking cessation in youth is understudied, several surveys suggest that there are few differences in cessation attempts and successful cessation by sex.70

Fig. 6: Trends in current-smoker prevalence among Canadian adolescents, 15–19 years of age. Source: Adapted from Gilmore.72
Although prevalence does not differ markedly by sex, girls and boys may smoke for different reasons. Among adolescent girls, body image, eating disorders and targeted advertising by tobacco companies likely relate to initiation of and sustained smoking, whereas aggression and conduct disorders appear to be fairly consistent predictors of smoking among boys.75 However, the current literature on sex differences in the determinants of smoking is generally inconclusive because many studies are cross-sectional, the definitions of smoking and of the potential determinants of smoking are widely divergent across studies and most studies investigated only small subsets of potential determinants.
Summary
• The prevalence of smoking is similar in girls and boys.
• Boys who smoke daily smoke more cigarettes a day than girls who smoke daily.
• Determinants of smoking differ with sex.
Knowledge gap
• The sex-specific incidence and prevalence of smoking should be monitored throughout the life course.
• Longitudinal life-course studies based on socioecologic models of health behaviour are needed to determine whether girls smoke for different reasons than boys.
• Researchers should examine the relative importance of individual (genetic, sociodemographic, psychosocial, behavioural) and environmental (social influences, policy, advertising) factors that influence smoking.
Diet
Dietary habits are important lifestyle behaviours that develop in early childhood. Although food consumption patterns have changed over the last several decades, no differences in these patterns have been noted between US boys and girls (except for the expected sex differences in mean energy intake [Fig. 7]).76,77 Carbohydrate consumption by children and adolescents has increased by 150–200 kcal/day (1 kcal = 4.184 kJ), while fat intake has decreased by 100 kcal/day or less.78,79 Significant increases in consumption of carbohydrates such as pizza and salty snacks have also been reported. The percentage of foods eaten at home has decreased, as more food is eaten in restaurants and fast-food chains.80 The prevalence of snacking has increased among youth of all ages — both portion sizes and frequency — accounting for the increase in average daily intake attributable to snacks.81
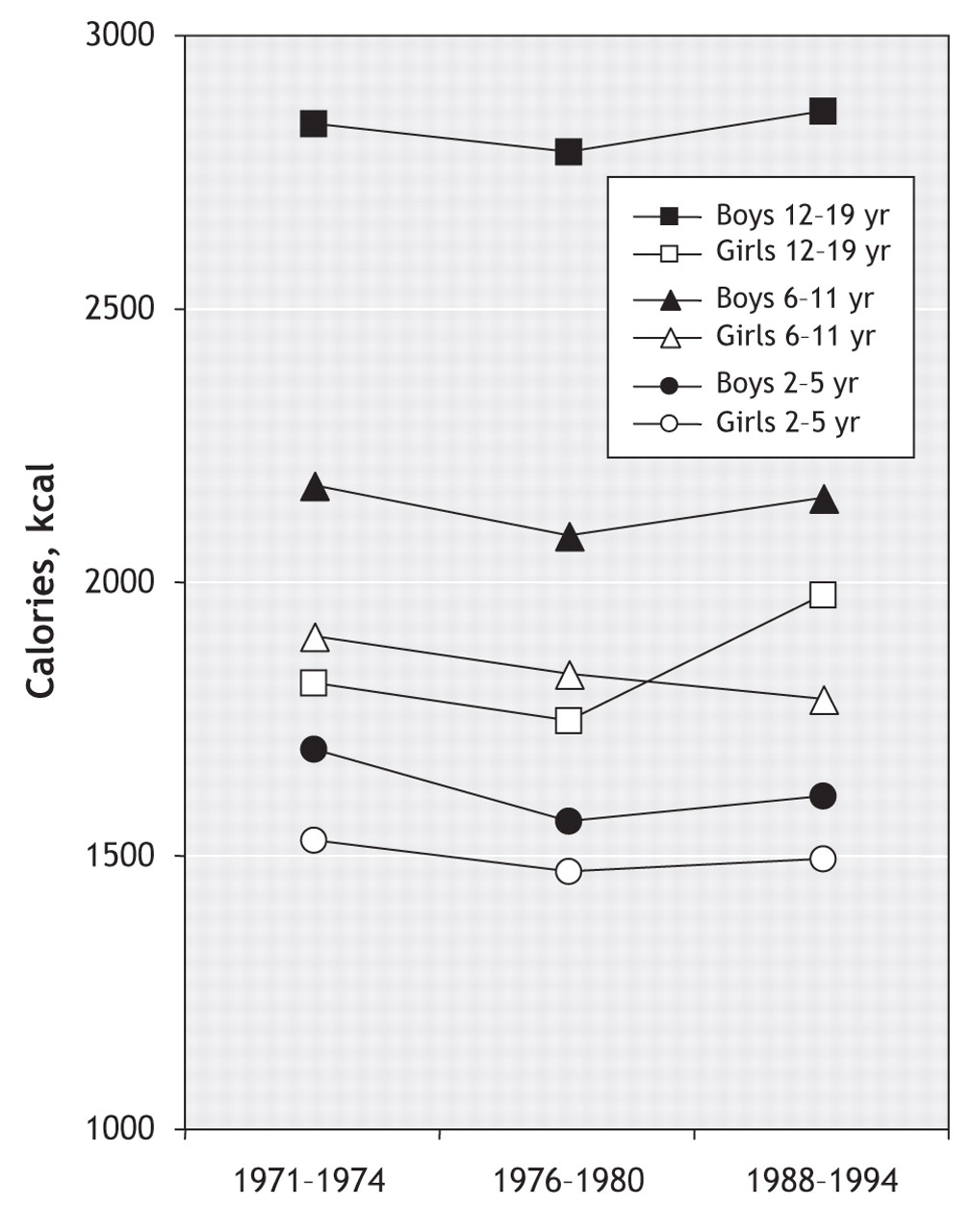
Fig. 7: Trends in mean daily caloric intake among children and adolescents. Source: Adapted from Troiano et al.77
There are fewer data available for Canadian children and adolescents, but the results of the few studies that have been conducted largely parallel US findings. A survey of 5th-grade children in Nova Scotia found that almost half do not meet the recommendations for consumption of milk products (42.3%) or fruits and vegetables (49.9%).82 Carbohydrate intake contributed 56.7% of total energy intake, of which 11% (32 g/day) was sucrose. Of the children, 13.9% exceeded the recommended range for fat intake (25%–35% of total calories). In 1 study that examined “diet quality” as an index of dietary variety, adequacy, moderation and balance, boys were found to have poorer diet quality than girls.82 In the Canadian Community Health Survey,71 57.8% of boys aged 12–19 years and 54.5% of similarly aged girls consumed less than 5 servings of fruit and vegetables a day. Eating at a fast-food restaurant more than 3 times a week was associated with a 56% increase in risk of lower diet quality. The Food Habits of Canadians study also provided data on food consumption patterns of adolescents based on 24-h dietary recall.83 These Canadian teenagers frequently consumed cakes, cookies, sweetened beverages, salty snacks and other nutrient-poor foods.
Several researchers have consistently found an increase in the consumption of sweetened beverages84 that is similar for boys and girls. Health Canada data from 1990 to 1998 indicate similar rates of consumption of soft drinks, colas and other drinks containing sugar for children aged 11, 13 and 15 years. Adolescents aged 11–16 years participated in the 2001–2002 Canadian component of the World Health Organization Health Behaviour in School-Aged Children Survey, which associated increased soft drink consumption with greater odds of overweight and obesity.85 Sweetened beverages contribute 20%–24% of energy to the diet of children and adolescents,77 and the percentage of total energy intake from soft drinks is greater among boys than girls.86 Milk consumption has decreased, although the decrease has been greater among boys.
Summary
• Total energy intake has remained largely constant over the past 4 decades with boys having an expected higher daily caloric intake than girls.
• Dietary patterns, including consumption of sweetened beverages and percentage of foods eaten outside the home, are similar for boys and girls.
• Boys and girls are eating more energy-dense, nutrient-poor foods in larger portions, a pattern that is consistent with the obesity epidemic.
Knowledge gap
• Researchers should evaluate socioecologic influences (e.g., parental dietary habits, psychosocial and behavioural factors, social influences, media and advertising) on dietary behaviour.
• Researchers should improve assessment procedures to determine more accurately children's dietary intake (advancing 24-h dietary recall, food frequency questionnaires and prospective food records or diaries).
• The sex-specific prevalence and trends in dietary and total energy intake should be monitored throughout the life course.
Physical activity and sedentary behaviour
Data from recent national surveys suggest a favourable trend in physical activity among Canadian adolescents.87 Between 1994 and 2003, the proportion of 12–19-year-olds classified as active (i.e., average energy expenditure ≥3.0 kcal/kg body weight a day) increased from 44.6% to 54.6% for boys and from 27.3% to 39.5% for girls. Despite this encouraging trend, the physical activity gap between boys and girls remains wide (Fig. 8).87 Girls report less physical activity than boys, both before and during adolescence.88–92 Sex differences are particularly apparent for vigorous physical activity, with girls less likely than boys to engage in such activity during their free time or in the context of organized physical activity, during school and outside school.93–95

Fig. 8: Trends in leisure-time physical activity among Canadian adolescents. Proportion active are those with an average daily energy expenditure of at least 3.0 kcal/kg. Source: Adapted from Statistics Canada.87
Although girls and boys are equally likely to be enrolled in organized physical activity and lessons outside school, girls are less likely to belong to sports clubs or participate in unorganized physical activity or in school sports outside physical education classes.96 Not surprisingly, boys and girls differ substantially in their physical activity preferences97,98 and in their patterns of involvement in physical activity.99,100 Boys and girls also differ in their attitudes and beliefs regarding physical activity,101,102 as well as their motivation for97,103 and barriers to104,105 engaging in physical activity.
Individual and environmental factors do not influence boys and girls equally.106,107 There is evidence that genetic effects are associated with sports participation and with leisure time physical activity to a greater extent in boys than in girls.108 Boys' and girls' physical activity levels are similarly affected by peer and family social support,109,110 but appear to be influenced by different neighbourhood factors. For example, perceived neighbourhood opportunities for physical activity are associated with girls' but not boys' activity levels,111 and physical features of the school environment appear to influence physical activity to a greater extent in boys.112,113 Finally, significant effects by sex are frequently observed in interventions promoting physically active lifestyles among youth.104,114
Data on sedentary pursuits are limited. A recent review concluded that total media use among youth in industrialized countries has remained stable in the past decades at approximately 5 h/day.104,115 The most recent data show that the proportion of adolescents aged 12–17 years who spend 30 h or more a week in sedentary activities (i.e., watching television, playing video games, spending time on the computer) is 30.0% in boys and 18.2% in girls.116 Most of the discrepancy between older boys and girls concerning time spent in sedentary pursuits relates to greater computer use and video game play in boys, not to television viewing.115,116
Sex and gender differences in physical activity and sedentary behaviour may be largely due to interactions between individual characteristics (e.g., physical maturation, personal motivation) and responses to environmental cues that enhance or inhibit involvement in these pursuits.
Summary
• Despite recent increases in physical activity in all youth, sex-related disparities in involvement in physical activity have not diminished.
• Boys are consistently more active than girls at all ages, and age-related decreases in physical activity occur earlier in girls than in boys.
• Most girls are not active enough to meet guidelines for optimal growth and development.
Knowledge gap
• Refine methods of physical activity assessment to capture the different dimensions and contexts of both sexes, including low-and moderate-intensity activities of daily living and active transportation, as well as the more traditional structured, free play and vigorous physical activities.
• Investigate the possible role of genetic inheritance in adaptation to sedentary or active lifestyles.
• Investigate how individual, familial, school and neighbourhood characteristics interact with sex and gender to determine involvement in physical activity.
• An increased understanding of the clustering of active and sedentary behaviours over the life course is required to help devise more effective sex-specific prevention and promotion programs.
Clustering of behavioural risk factors
According to the Canadian Cardiovascular Society's 1998 consensus on the prevention of CVD, the major CVD behavioural risk factors in youth include smoking, physical inactivity and obesity.117 These modifiable risk factors persist from childhood into adulthood41–44 and tend to cluster among youth.118–121 In the longitudinal Cardiovascular Risk in Young Finns Study, Raitakari and colleagues118 found that 15- and 18-year-old boys and girls who smoked were more likely to be regular users of alcohol and physically inactive compared with non-smokers. Obesity was more prevalent among physically inactive compared with active males (14% v. 8%, p < 0.05), female drinkers compared with non-drinkers (20% v. 9%, p < 0.001) and smokers compared with non-smokers (males 15% v. 9%, p < 0.05; females 16% v. 9%, p < 0.01). In males, those with 4 selected CVD behavioural risk factors, including smoking, physical inactivity, obesity and intake of dietary fat, had a 5.5 times greater risk of having an atherogenic lipid profile and high diastolic blood pressure compared with those with 0 or 1 behavioural risk factor.118 In another prospective study investigating the association between family socioeconomic status and an adverse cardiovascular risk profile among 14- and 17-year-old boys and girls in Sweden, Bergstrom and colleagues119 reported clustering of high BMI, low physical fitness and daily smoking among girls living in families of low socioeconomic status compared with girls of the same age in families of medium or high socioeconomic status.
In the United States, Pate and colleagues120 investigated the association between physical activity and other health-related behaviours, including smoking and dietary habits, in a representative sample of adolescents aged 12–18 years. Boys and girls who smoked 1 or more cigarettes over the past 30 days and who did not eat fruits or vegetables on the previous day were 1.5 and 2 times more likely to be less active than those who did not report these behaviours, respectively. In a more recent study, Pronk and colleagues121 reported that only 31% of US adolescents aged 13–17 years met recommended guidelines for multiple healthy lifestyle factors including physical activity, non-smoking, high-quality diet and healthy weight. This implies that more than two-thirds of US adolescents have 1 or more CVD behavioural risk factors, an estimate that is quite alarming given the potential synergistic effects associated with the presence of multiple behavioural risk factors on the risk of chronic diseases in adult life.122 Pronk and colleagues121 also found that depression is associated with clustering of health-related behaviours in adolescents. Specifically, non-depressed adolescents were 2.15 times more likely to engage in 4 healthy lifestyle factors. The clustering of health-related behaviours in US adolescents was similar for boys and girls.
Data on the prevalence and potential determinants of multiple CVD behavioural risk factors in Canada are scarce. The studies reviewed in this section suggest that CVD behavioural risk factors cluster in children and adolescents. Certain sociodemographic characteristics, including age and sex,109,110 and psychosocial variables, such as depression and family socioeconomic status,112 seem to be associated with the clustering of CVD behavioural risk factors in youth, but evidence in this area remains limited and inconsistent.
Critical analysis of studies
All the studies reviewed were observational, cross-sectional cohort or longitudinal studies. Wherever possible, results of studies specifically focusing on girls or on boys or providing sex comparisons have been included. The areas not sufficiently addressed by existing studies have been highlighted as knowledge gaps.
Why are there sex differences?
When sex differences in risk factors are apparent, they appear to be attributable to a combination of biologic (sex) and behavioural (gender) factors. Compared with age-matched boys, girls have lower systolic blood pressure. However, this sex difference is attenuated with age and may be partly attributable to sex hormones or their receptors. In terms of health behaviours, the prevalence of smoking does not differ markedly by sex, although boys smoke more cigarettes a day than girls, and they are more likely than girls to escalate cigarette consumption rapidly after initiation. Boys and girls appear to smoke for different reasons. Body image, eating disorders and targeted advertising by tobacco companies likely relate to initiation and sustained smoking among adolescent girls, while aggression and conduct disorders are predictors of smoking among boys. Sex differences in physical activity are also apparent; girls are less likely to engage in physical activity than boys, both before and during adolescence. This may be partly due to sex and gender factors.
Summary
• The major CVD behavioural risk factors, including smoking, physical inactivity and obesity, cluster among young boys and girls.
• Having multiple CVD behavioural risk factors increases the risk of atherogenic profile and high blood pressure among boys.
• Age, gender, depression and family socioeconomic status are associated with clustering of CVD behavioural risk factors in youth.
Knowledge gap
• Studies identifying the prevalence and determinants of multiple CVD behavioural risk factors in youth are warranted.
• A better understanding of the frequency and clustering patterns of CVD behavioural risk factors in young girls and boys is needed to facilitate health professionals' efforts to reduce the incidence of CVD.
Cardiovascular risk factors in women and men
Kaberi Dasgupta, Susan Kirkland, Doreen Rabi and Vicky Tagalakis
The Framingham Heart Study established the independent impact of cigarette smoking, elevated blood pressure, elevated total cholesterol and LDL cholesterol, low HDL cholesterol, diabetes, male sex and advancing age on the development of CVD.123 Based on Framingham cohort data, equations for the calculation of risk of CVD have been developed and treatment targets for blood pressure and lipid levels are now dictated by global recommendations.124,125
Excess weight and physical inactivity have an adverse impact on blood glucose levels, blood pressure and lipid profiles.126 Individuals in the Framingham cohort who lost at least 2.25 kg over 16 years had a 40%–50% reduction in their total cardiovascular risk factor score.127 Independent of its impact on weight, regular exercise has favourable effects on glucose control, blood pressure, serum lipids and fitness levels.126,128–133 Higher fitness levels have been demonstrated to be independently associated with a reduction in CVD events and mortality.134,135
A number of additional markers of risk for CVD have been identified, including biomarkers, such as C-reactive protein and plasminogen activator inhibitor type-1, and demographic factors, such as low socioeconomic status. It remains to be determined whether such markers are independent risk factors, predisposing or intermediary factors associated with established risk factors, or noncausally associated with CVD.
Although Framingham data indicate that men are generally at increased risk for CVD than women, the distribution and impact of other CVD risk factors and markers may also differ between men and women, with implications for prevention, detection and management of CVD in both sexes. In this section, we review the existing literature regarding sex differences in the prevalence and impact of overweight and obesity, physical activity, hypertension, diabetes, smoking, dyslipidemia, selected cardiovascular risk markers and socioeconomic factors.
Search strategy
Boolean searches of MEDLINE from 1966 to August 2005 were performed by combining the MeSH term “cardiovascular disease” with each of the following MeSH terms: “obesity,” “physical activity,” “hypertension,” “diabetes,” “socioeconomic status,” “smoking,” “C-reactive protein,” “homocysteine,” “apolipoprotein E,” “dyslipidemia,” “fibrinogen,” “plasminogen activator inhibitor type-1” and “lipoprotein (a).” Each of these searches was combined using the term “AND” with a search that used the terms “gender” and “sex” and the term “OR.” Searches were restricted to English-language publications, but no other restrictions applied. In addition, the references of the resulting publications were hand searched for further articles.
Overweight and obesity
Obesity-related complications include
• Vascular risk factors — Hypertension, dyslipidemia and type 2 diabetes
• Vascular disease — Ischemic heart disease, hypertensive heart disease, stroke, renal failure, peripheral vascular disease and retinopathy
• Other conditions — Osteoarthritis, malignancy (breast cancer), depression and polycystic ovary syndrome
Sex differences in prevalence of overweight conditions
In the United States, data from NHANES indicate that the overall prevalence of overweight (BMI ≥ 25 kg/m2) was 55.9% in 1988,136 rising to 64.6% by 1999.137 Data from the Canadian Community Health Survey indicate that the prevalence of overweight remained stable at 48% between 1994/95 and 2000/01 in the population aged 20–64 years, although 2% of individuals shifted from the overweight (BMI 25–30 kg/m2) to the obese (BMI ≥ 30 kg/m2) category.138
Sex differences in overweight and obesity are influenced by geography and ethnic background (Table 6). For example, among white and Mexican Americans, the prevalence of overweight is higher among men than among women. However, among black Americans, the prevalence of overweight is higher among women than men. The prevalence of obesity is higher among US women than men, with the highest prevalence among black American women.139
Table 6.
In Canada, for both men and women, the prevalence of overweight is lower among black Canadians (50%) than white Canadians (60%).140 Consistent with this, among men, the prevalence of obesity is lower among black Canadians (10%) than white Canadians (15%), although among Canadian women, the prevalence of obesity is higher among black people (20%) than white people (15%). The ethnic group with the highest rates of overweight and obesity is the Aboriginal population (60% overweight in women and 65% in men; 25%–30% obesity in men and women). Between 1994/95 and 2000/01, the prevalence of obesity increased in all age and sex groups in Canada, with the exception of women 20–34 years of age. These trends are consistent with those documented in other countries.141–144
Overweight and obesity are also prevalent in many developing countries. Nishida and Mucavele145 found that the prevalence of obesity was higher in women than in men in the following countries: Brazil, 11.7% v. 4.8%; Egypt, 33.0% v. 12.6%; South Africa, 30.1% v. 9.4%; Seychelles, 28.2% v. 8.5%. The prevalence of overweight was similar for the 2 sexes, but countries reporting higher levels of overweight among women were located in Africa, Latin America, Asia and Oceania, whereas male overweight was more prevalent than women's in countries of Europe and North America.
Recommendations for the prevention and treatment of obesity
• Reduced consumption of energy-dense foods
• Regular physical activity
• Weight loss for those with BMI ≥ 25 kg/m2 (diet and exercise counselling, behavioural counselling)
• Those with BMI ≥ 35 kg/m2 or with BMI ≥ 30 kg/m2 and obesity-related complications may consider bariatric surgery
Periods of risk
Women appear to be particularly susceptible to significant weight increase during adolescence,146 pregnancy136 and menopause.147 The weight increase that occurs during menopause has been shown to be associated with a significant increase in blood pressure.148 The period after marriage appears to be a period of risk for weight gain among men.149
Knowledge gap
• Does the utility of weight loss for the prevention of CVD differ between women and men?
• Why do obese people appear to have lower rates of fatal recurrent cardiovascular events?
• What weight-loss strategies are particularly effective among men?
• What weight-loss strategies are particularly effective among women?
• Why are black women in both the United States and Canada at high risk of obesity?
Physical activity
Sex differences in activity levels
Many studies suggest that women are more likely to be sedentary than men. A questionnaire administered by Pitsavos and colleagues150 in the Attica region of Greece revealed that, overall, 53% of men and 48% of women were physically active, and men tended to be more physically active than women across all age groups. In an interview-based survey conducted in Portugal, 79% (95% CI 75.7–81.6) of men and 86% (95% CI 84.0–88.0) of women were found to be sedentary.151 In Finland, the proportion of people classified as sedentary or only moderately active during their leisure time was 75% among males and 82% among females.152 Men in Japan have also been found to be more active than women.153
There is some evidence that, although both men and women are both less likely to be active when weather conditions are unfavourable, women are less likely to increase activity levels when weather conditions become more favourable. In community-dwelling adults in Massachusetts, mean physical activity during the summer increased by 51 minutes/day (95% CI 20–82) in men, but only by 16 minutes/day (95% CI -12–45) in women.154
Potential mechanisms
Low levels of physical activity render weight maintenance difficult, contribute to the development of insulin resistance, with associated increases in blood pressure, blood glucose level, dyslipidemia and thrombogenic factors. In addition, there is increasing evidence that low levels of activity and fitness are directly related to increased CVD risk. In a prospective cohort study that examined the impact of physical activity on mortality, Blair and colleagues155 found that women in the lowest tertile of physical activity had a greater than 5-fold increased risk of mortality compared with women in the highest physical activity tertile. Men in the lowest physical activity tertile were at a 3-fold higher increase in risk of mortality compared with men in the highest fitness tertile.
Barriers to physical activity in women
Findings from Canada's National Population Health Survey demonstrate that the presence of children in the household is a significant deterrent to becoming active for women, but not for men.156 The most commonly reported barrier to women's participation in physical activity is lack of time due to family responsibilities.157,158 Middle-aged and older women appear to have positive attitudes toward exercise, but are unable or unwilling to take action.159
Physical activity recommendations
• To remain healthy and maintain body weight — moderate exercise (e.g., walking) 30 minutes daily or vigorous exercise (e.g., jogging) 20 minutes daily.
• To lose weight — vigorous exercise 30 minutes daily.
Knowledge gap
• What are the barriers to physical activity in women?
• Are the barriers largely related to child care or competing work–home responsibilities or both?
• How can activity levels among women be increased?
Hypertension
Excess body weight and physical inactivity may promote the development of a number of CVD risk factors, including high blood pressure (see Table 7 for the general classification of blood pressure levels).
Table 7.
Hypertension-related comorbidities
• ischemic heart disease
• hypertensive cardiomyopathy
• stroke
• renal failure
Sex differences in blood pressure
In the third NHANES (1988–1994) evaluation, among US adults under 45 years of age, men had higher systolic blood pressure levels than women.160 By 60–69 years of age, non-Hispanic white women had blood pressure levels similar to those of men and by 70–79 years of age, had higher levels than men.161 By 60–69 years of age, non-Hispanic black and Hispanic women had higher blood pressure levels than men of similar ethnic background.161 Overall, among those 45 years of age and older, systolic blood pressure levels were higher among women.160 In a cohort study conducted in Denmark, 24-h mean blood pressure levels were 6–10 mm Hg higher among men than women until 70–79 years of age, but similar thereafter.162 Women from developing countries have higher mean systolic blood pressure than their male counterparts.163 It is also noteworthy that women from these countries have higher blood pressure than women from developed countries. Women from the African region have the highest mean systolic blood pressure.
Among young and middle-aged adults, population surveys report hypertension to be more frequent among men compared with women, with sex differences of 4% in the United States, 8% in Canada and 11% in Western Europe.164 After 60 years of age, however, the prevalence of hypertension appears to be higher among women than among men.
Potential mechanisms
Androgen is thought to play a role in the sex differences in blood pressure. One possible mechanism may be the blunting of the pressure-natriuresis relation.165 Female sex hormones and their receptors may also be implicated in blood pressure differences between men and women. A genetic association study by the Victorian Family Heart Study investigators found that men inheriting the “a” allele on the estrogen receptor a gene had significantly higher systolic blood pressure levels (5 mm Hg) than men with other genotypes.166 No significant associations between estrogen receptor genes and blood pressure were detected among women.
Knowledge gap
• How can the postmenopausal increase in hypertension be prevented?
• Should the threshold for hypertension diagnosis in women be lower to prevent the postmenopausal increase in hypertension?
• Can earlier detection of hypertension in boys and young men reduce the sex–gender differential in incidence of CVD between men and premenopausal women?
Diabetes
Diabetes is highly prevalent; over 151 million people live with this condition worldwide (Table 8). Diabetes is an established risk factor for the development of CVD.167 People with diabetes have a 2- to 4-fold greater risk of developing CVD compared with those without diabetes.168 CVD is the leading cause of morbidity and mortality for those living with diabetes.
Table 8.
Although the prevalence of diabetes is lower in developing countries, these countries have experienced the greatest increase in diabetes. The prevalence is highest in the Eastern Mediterranean and Middle East (7.0%), South and Central America (5.6%), Southeast Asia (5.6%), Western Pacific (3.1%) and Africa (2.4%). The prevalence of diabetes is higher among women than among men in Latin America (57.5% v. 42.5%) and in the Western Pacific (53.7% v. 46.3%).169
Diabetes-related vasculopathy
Microvasculature
• retinopathy
• nephropathy
Macrovasculature
• peripheral vascular disease
• cerebrovascular disease
• ischemic heart disease
Because CVD is more prevalent among men, it follows that most studies that have examined the significance of diabetes as a risk or prognostic factor have predominantly male participants. However, Hu and colleagues170 examined the prognostic significance of diabetes in their analysis of the Nurse's Health Study Cohort and found that women with diabetes had surprisingly high cardiovascular-related mortality. This study demonstrated that the adjusted relative risk (RR) for cardiovascular-related death among women who had established CVD, after controlling for other vascular risk factors, such as smoking status, family history of ischemic heart disease and BMI, was 13.6 (95% CI 8.45–21.8). However, it should be noted that there was no control for differences in hypertension, hypercholesterolemia or socioeconomic status, risk factors that are well known to be more prevalent among both women and men with diabetes.
Diabetes as a prognostic factor among patients with CAD
Although diabetes is an established risk factor for the development of CVD, the significance of diabetes as a prognostic factor following an ischemic event remains less clear. Numerous studies have demonstrated that patients with diabetes appear to have poorer clinical outcomes following myocardial infarction (MI), stroke and percutaneous and surgical revascularization compared with non-diabetic patients. However, in a prospective cohort study of 11 468 patients presenting for coronary catheterization (17% of whom had diabetes), Ghali and colleagues171 demonstrated that, after controlling for all clinically relevant variables, the survival of patients with diabetes was the same as for those without diabetes at 1 year (OR 1.1; 95% CI 0.8–1.3) and 3 years (HR 1.2; 95% CI 1.0–1.4).
Graham and colleagues172 completed a large prospective cohort study examining sex differences in the prognostic significance of diabetes following coronary catheterization. After adjusting for several clinical variables, they demonstrated a trend toward increased mortality in women with diabetes, although this was not statistically significant. Several systematic reviews and meta-analyses have been carried out to determine the association between sex and CVD mortality.173–175 Lee and colleagues173 found that women with diabetes had a relative risk of coronary death from diabetes of 2.58 (95% CI 2.05–3.26) compared with non-diabetic women, which was significantly higher than for men with diabetes (RR 1.85; 95% CI 1.47–2.33). This review was limited in that the included studies had variably controlled for other coronary risk factors. When Kanaya and colleagues174 reviewed studies that adjusted for age, hypertension, hyperlipidemia and smoking status, they found that there was no longer a significant difference in cardiovascular-related mortality between men and women with diabetes. Reviewing data from North America, Europe and the Asian Pacific Cohort Studies Collaboration, Huxley and colleagues 175 found, like Lee and colleagues, that women with diabetes had a 3.5-fold (95% CI 2.7–4.5) increase in CVD mortality compared with non-diabetic women and that this was significantly higher than for their male counterparts (RR 2.1; 95% CI 0.81–2.34). Sensitivity analyses that corrected for coronary risk factors revealed that this sex difference was attenuated, but remained statistically significant (Table 9).
Table 9.
A recent cohort study demonstrated that a history of diabetes in women was associated with a 37% increase in CVD-related mortality compared with a history of AMI. However, the presence of a previous AMI in men increased the risk of CVD-related mortality by 43% compared with a history of diabetes.176
Potential mechanisms
Several mechanisms may explain the apparent sex difference in CVD mortality among patients with diabetes. There is evidence that different pathophysiologic processes — in terms of endothelial function, dyslipidemia and thrombosis — may result in different cardiovascular outcomes among men and women with diabetes.
Diabetes has been shown to abrogate the vascular protection afforded to premenopausal women. Steinberg and colleagues177 elegantly demonstrated that premenopausal women have an enhanced vasodilatory response to endogenously produced nitric oxide compared with men. This study also illustrated that the development of diabetes is associated with abnormal endothelial-dependent vasodilation in both sexes. This loss of vasodilation is most striking in women. Sowers178 has further demonstrated that hyperglycemia significantly decreases estrogen-mediated nitric oxide production. It seems that a unique interaction between diabetes and sex makes women more vulnerable to endothelial dysfunction.
The noted sex differences in CVD outcomes may be influenced by factors beyond biology. A study by Wexler and colleagues179 suggests that sex differences in CVD mortality may be due to disparities in medical management. This prospective cohort study demonstrated that women with diabetes were less likely to be treated until they reached established therapeutic targets than men with diabetes, even if the women had established CVD. Whether these disparities are related to physician factors (underappreciation of cardiovascular risk in women, hesitation to use vasoprotective medications in reproductive women) or patient factors (adherence to or tolerance of prescribed medications) remains unclear.
Dyslipidemia
Abnormal levels of lipoprotein cholesterols are significant predictors of atherosclerosis in all populations, with a fifth of global stroke events and about 56% of global heart disease attributable to high cholesterol levels. In particular, elevated levels of total cholesterol, LDL cholesterol and triglycerides and low levels of HDL cholesterol have been associated with CAD, stroke and peripheral vascular disease and are often associated with such significant comorbidities as diabetes, hypertension and obesity. In both US and Canadian populations, abnormal cholesterol levels are highly prevalent across different age and ethnic groups (Table 10 and Table 11),180 and there appear to be sex differences in the prevalence of elevated cholesterol181,182 (see Table 12 for classification of lipoprotein levels).
Table 10.
Table 11.
Table 12.
Low-density lipoprotein
LDL cholesterol is believed to be the principal lipoprotein in the development of atherosclerosis and remains the primary target of therapy for the prevention of CVD. Elevated LDL cholesterol levels are more predictive of coronary risk in men than in women, particularly premenopausal women.183 This might be due in part to lower levels of LDL cholesterol in premenopausal women than in middle-aged men (35–65 years). However, after age 50 years, LDL cholesterol levels plateau in men and increase in women between ages 40 and 60 years at an average rate of 0.05 mmol/L a year.184 This increase in LDL cholesterol at menopause is thought to be partly the result of advancing age and declining levels of estrogen, which result in downregulation of LDL receptors in the liver leading to decreased clearance of LDL cholesterol from the serum.
High-density lipoprotein
HDL cholesterol is an important independent predictor of CVD in both men and women,185,186 but may have greater predictive potential in women than men.185,187 In the Framingham Heart Study, a 0.025-mmol/L increase in HDL cholesterol level was associated with a 3% decrease in the incidence of CAD in women compared with a 2% decrease in men.185 In the Lipid Research Clinics Prevalence Mortality Follow-up Study, a 0.025-mmol/L increase in HDL cholesterol was associated with a 4.7% reduction in CVD mortality among women (p = 0.002) compared with a 3.7% reduction among men (p < 0.001).188 On average, HDL cholesterol levels are 0.25 mmol/L higher in premenopausal women than in men, which may account for the lower incidence of CVD before age 50 in women compared with men. With menopause, HDL cholesterol levels have been shown to decrease, although the administration of exogenous estrogen can increase levels.189 However, the protective effect of exogenous estrogens remains controversial. Although oral estrogens can increase HDL cholesterol and decrease LDL cholesterol, they also increase the potential for coagulation and possibly for inflammation.
Triglycerides
There is some evidence to suggest that high levels of triglycerides are a significant independent risk factor for CVD in both sexes, but more so in women than men.185,190 In a meta-analysis of 17 prospective population-based studies, elevated triglyceride levels adjusted for HDL cholesterol levels were associated with a 37% (95% CI 13–66) increase in risk of CVD-related events in women compared with a 14% (95% CI 5–28) increase in men.191 The mechanism for increased risk of CVD associated with hypertriglyceridemia is unclear, but elevated triglycerides are often accompanied by other metabolic disturbances that may predispose to CVD, including reduced HDL cholesterol, increased levels of very low-density lipoprotein cholesterol and insulin resistance, which makes it difficult to assess the independent risk associated with triglycerides. Moreover, some analyses suggest that elevated triglycerides interact with some of these other risk factors to modulate the risk of CVD and that the interaction may differ between men and women. For example, a study of 174 patients with type 2 diabetes mellitus who were not receiving lipid-lowering therapy concluded that the severity of CAD (as examined by angiography) was related to the number of triglyceride-rich lipoproteins and that the relation was stronger for women than men, independent of HDL and LDL cholesterol.192
Knowledge gap
• Triglyceride and HDL cholesterol levels must be measured and addressed, especially in women with other metabolic disturbances.
• Changes in triglycerides, HDL cholesterol and other lipid metabolites may be indicators of unrecognized metabolic disturbances, especially in women.
• Pharmacologic interventions to elevate HDL cholesterol in women have not been undertaken.
Smoking
Smoking has been identified as the primary preventable cause of morbidity and mortality in Canada, contributing to 27% of all deaths among men and 17% of all deaths among women, the majority being due to CVD.193 Trends in smoking-attributable mortality reflect the smoking behaviour of the population 2–3 decades earlier. Whereas smoking rates for men peaked in the mid 1960s, the rates for women did not begin to decline until the late 1970s. As a result, deaths due to CVD among women have yet to decrease.193,194
Ongoing national and provincial surveillance initiatives monitor smoking trends and the effect on health. Smoking prevalence has steadily declined over the last few decades, with a stronger decrease in men than women (Fig. 9).195 According to the 2004 Canadian Tobacco Use Monitoring Survey (CTUMS),196 approximately 22% of men and 17% of women aged 15 years and older are current smokers. Although women experiment with smoking at a younger age than men, smoking rates are higher for men than women in all age groups. Prevalence peaks at ages 20–29 years in both sexes — at 37.3% in men and 30.9% in women. For both sexes, the prevalence begins to decline at age 30–49 years and smoking prevalence among those aged 55 years and older is half that of 20–29 year olds.195,197,198 The overall smoking rate of 20% is among the lowest in the OECD countries and is favourably consistent with trends in other developed countries. However, we may have reached a point at which the prevalence rates reflect hard-to-reach populations, and further decreases may be difficult to achieve. In a survey similar to CTUMS conducted in the Northwest Territories, the prevalence of smoking was 44% and 38% among men and women, respectively, yet Aboriginal residents had a prevalence of over twice that of non-Aboriginal residents, 60% v. 25%.199
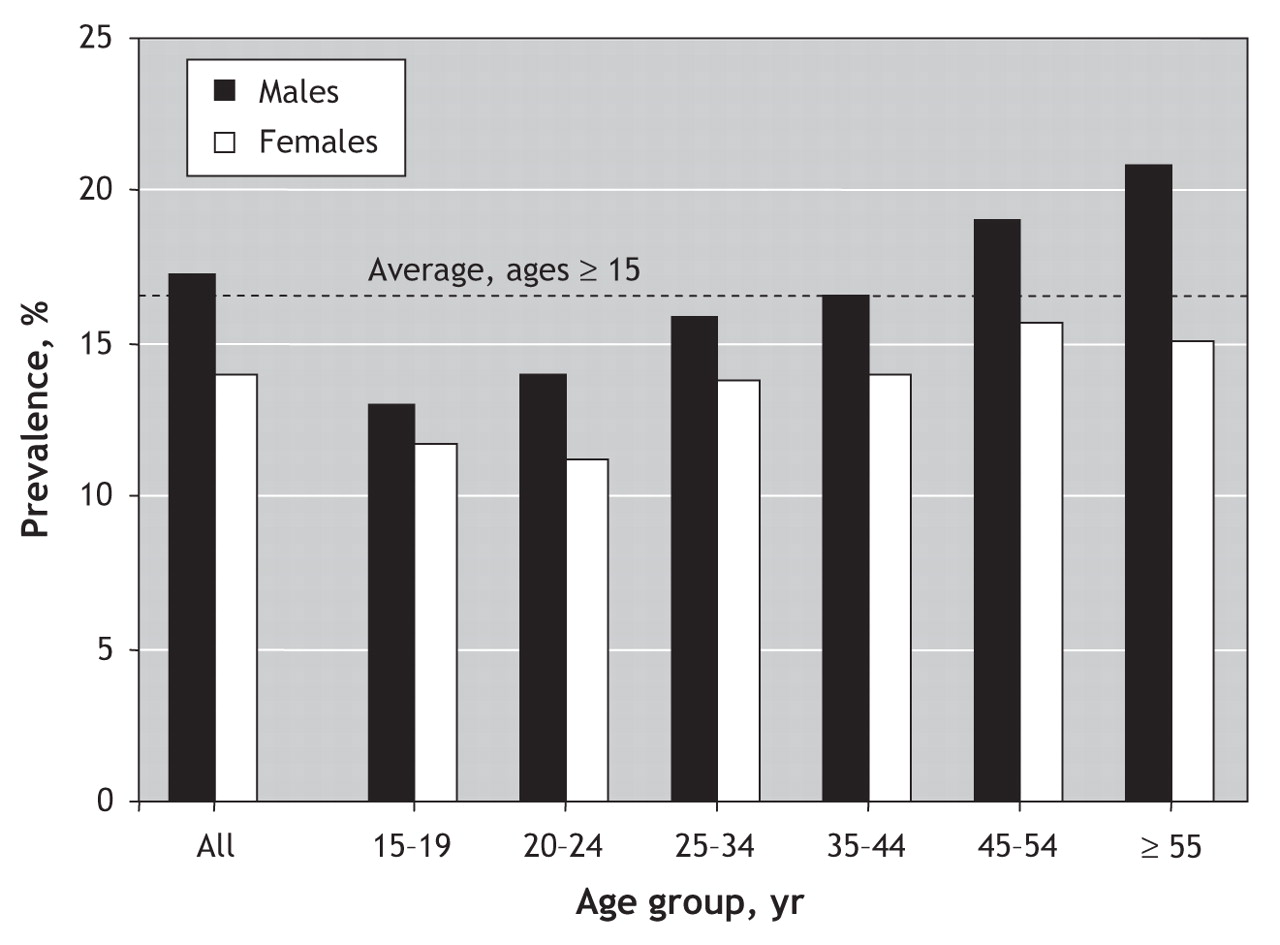
Fig. 9: Prevalence of current smoking by age and sex, 2003. Source: Adapted from Canadian Tobacco Use Monitoring Survey.195
In developing countries, the prevalence of smoking is substantially higher among men (50%) than among women (9%). However, female smoking is increasing rapidly due, at least in part, to targeted promotional strategies of the tobacco industry. Worldwide, the lowest smoking prevalence for both men and women is in African countries, while the highest prevalence for men is in Eastern Europe (where rates exceed 60%) and for women in Central Europe and parts of South America.200 The greatest increases in smoking prevalence over the next decade are expected to occur in Africa and the Middle East.
The determinants of smoking primarily reflect social and economic disadvantage. A higher prevalence of smoking has been found among women and men who live in low-income households, have low-status jobs or are unemployed, are single parents or divorced, and have low levels of education.194,201 This is consistent with the epidemic description of smoking as it spreads through a population, reverting from a positive association to a negative association with socioeconomic status, first among men and then among women in later stages of the epidemic, as seen in developed countries.202 Qualitative research has shown that men and women may smoke for different reasons. For example, women use smoking as a coping mechanism to deal with gendered stresses such as child care.203 They may also encounter greater difficulties in quitting.199
Epidemiologic studies have consistently documented the risk of CVD associated with smoking in both sexes. It is generally thought that the CVD risk is similar, except among women smokers taking oral contraceptives, where the risk of stroke is much greater. However in ARIC, a large prospective population study of 15 792 men and women aged 45–64 years at entry, investigators found that the hazard ratio for coronary heart disease was greater for women than men (2.95 v. 1.55 for current smoking).204
Potential mechanisms
The precise mechanisms connecting increase in CVD risk with smoking are not completely clear. Possible deleterious impacts of smoking include endothelial dysfunction, lipid abnormalities, increased concentration of fibrinogen and platelet aggregation.205,206 Few studies have investigated the possible mechanisms underlying sex differences in CVD associated with smoking. Interactions between smoking and hormonal factors may be involved in development of CVD. It is possible that smoking may increase the risk of CVD in women smokers via an anti-estrogenic effect.205
Cardiovascular risk markers
C-reactive protein
Inflammatory mechanisms have been shown to play an important role in the pathogenesis of CVD, and increasing attention has been paid to the measurement of inflammatory biomarkers, particularly C-reactive protein (CRP).207–209 Indeed, of 12 plasma markers evaluated simultaneously, Ridker and colleagues207 found CRP to be the most significant predictor of CVD risk in healthy postmenopausal women. Adjusted for other plasma markers and conventional risk factors, a 1-quartile increase in CRP concentration increased the risk of a CVD event by 50% (OR 1.5; 95% CI 1.1–2.1). These findings were supported in a meta-analysis of 22 prospective studies conducted in general (apparently healthy) populations.208 Those in the top third of the study group, with respect to CRP level, had a 58% increase (OR 1.58; 95% CI 1.48–1.68) in risk of CAD compared with the bottom third, after adjusting for the major conventional CVD risk factors. Although most studies were predominantly in men, the summary odds ratio reported separately for women in 3 studies did not differ markedly from the summary odds ratio based on 12 studies that reported their findings for men only. Studies in groups with established heart disease have also demonstrated that high CRP levels are associated with increased AMI or mortality.210
A number of other studies have reported higher adjusted baseline CRP values for women than men.209,211 Bertran and colleagues211 found that, on average, CRP concentrations were 29% higher in women than men. An age–sex interaction has also been demonstrated, whereby CRP was predictive of death or AMI, or both, in women and men under 55 years of age, but only for men over the age of 55 years.209
Homocysteine
Elevated levels of homocysteine have also been implicated in CVD. Blood levels of homocysteine have been found to be higher in men than in women.212,213 For example, homocysteine levels in the control group were 9.7 ± 4.9 μmol/L for men and 7.6 ± 4.1 μmol/L for women (p < 0.001) in a case– control study of French-Canadians.213 Men and women with CAD had significantly higher homocysteine levels (11.7 ± 5.8 μmol/L and 12.0 ± 6.3 μmol/L, respectively), but no sex difference in CAD was observed.
A systematic review214 of the association between plasma homocysteine level and CVD suggested that moderately increased homocysteine levels are prevalent in the general population and are independently associated with an increased risk of CVD. In a more recent meta-analysis,215 elevated homocysteine level was found to be a modest independent predictor of ischemic heart disease in healthy populations; a decline of 3 μmol/L in homocysteine level was associated with an 11% decrease in risk of ischemic heart disease (OR 0.89; 95% CI 0.83–0.96).
Apolipoprotein E
Apolipoprotein E (APOE) is a component of lipoproteins, with considerable variation as a result of cysteine–arginine exchanges in 3 alleles known as ε2, ε3 and ε4. Numerous population studies have implicated APOE as a major modulator of total cholesterol and LDL cholesterol.216–218 The presence of the ε4 allele has been associated with elevations in LDL cholesterol, whereas the ε2 allele has been associated with decreased levels of LDL cholesterol.216–218 Data from the Framingham Offspring Study have also indicated that the association of APOE phenotype with LDL cholesterol level is significantly greater in postmenopausal women than in premenopausal women or in men.218
Some studies have indicated that the APOE polymorphism may be a sex-specific predictor of CVD.219,220 Most recent data from the Framingham Heart Study suggest an increased risk in men with the ε2 and ε4 alleles compared with those with the ε3:ε3 genotype. After adjustment for all risk factors including age and lipids, the increase in risk of CVD with an ε4 allele was 51% for men (OR 1.51; 95% CI 1.05–2.18) and 48% for women (OR 1.48; 95% CI 0.93–2.34). The association between the ε2 allele and CVD remained significant in men after adjusting for all risk factors, including lipids (OR 1.94; 95% CI 1.23–3.04). However, no association between the ε2 allele and increased CVD risk was found in women.219 Neither the mechanism underlying the excess in ε4 allele in CVD patients nor the effect of interaction between sex and APOE polymorphisms on CVD is completely clear.
Fibrinogen
Increased plasma fibrinogen levels have been independently associated with an increased risk of AMI and stroke in prospective studies of healthy people and patients with pre-existing CVD.221–223 Both men and women in the highest third for plasma fibrinogen have a 2- to 3-fold higher risk than those in the lowest third.224 In a meta-analysis of 31 prospective studies that included 154 211 participants from Western Europe, North America and Japan, the age-and sex-adjusted hazard ratio per 1-g/L increase in usual fibrinogen level was 2.42 (95% CI 2.24–2.60) for coronary heart disease and 2.06 (95% CI 1.83–2.33) for stroke.225 Although the risk of CVD is similar for men and women with elevated fibrinogen levels, there are some small sex differences with regard to modulators of fibrinogen levels; women tend to have higher levels of fibrinogen than men when stratified for age and ethnicity.226,227 Plasma fibrinogen increases with menopause, pregnancy and the use of oral contraceptives; treatment with hormone replacement therapy may decrease fibrinogen levels, and the effect of smoking, which is regarded as the strongest determinant of high fibrinogen levels,226 is not as consistent in women as it is in men.228,229 Possible reasons include differences in nutritional habits and more powerful determinants of fibrinogen in women, such as hormonal status, that could mask the smoking effect. Although the clinical significance of these sex differences remains to be elucidated, they may be useful in the development of sex-specific interventions to lower fibrinogen levels.
Plasminogen activator inhibitor type-1
Increased levels of plasminogen activator inhibitor type-1 (PAI-1) have been associated with CAD.223,230–232 In a recent prospective nested case–control study of 2246 Swedish patients with a first AMI matched for age and sex, elevated levels of PAI-1 were significantly associated with a 2-fold increased risk of AMI in both men and women.233 A few studies have shown that premenopausal women have lower plasma PAI-1 levels than postmenopausal women.234 In addition, postmenopausal women receiving hormone replacement therapy have lower plasma PAI-1 levels than those not receiving such therapy.235,236
The presence of polymorphisms in the PAI-1 gene has been found to correlate with increased plasma levels of PAI-1 and may help explain differences among men and women and even among pre-and postmenopausal women. For example, a large cohort study of men and women with recent AMI revealed that the risk of AMI, after adjusting for common CVD risk factors, was significantly associated with 4G/5G polymorphism in women compared with men.237 More recently, a few case–control studies have shown a higher prevalence of this mutation in postmenopausal women with CAD compared with premenopausal women with and without CAD, and the addition of hormone replacement therapy decreases PAI-1 levels in women with CAD, which correlates with the presence of the 4G allele.238
Lipoprotein (a)
Lipoprotein (a) (Lp(a)) has been postulated to be highly atherothrombotic. A recent meta-analysis of 18 prospective population-based studies, which included over 3500 women, largely from Nordic countries, Germany, the United Kingdom and the United States, showed a combined risk ratio for CVD of 1.7 (95% CI 1.4–1.8) for those in the top third of baseline Lp(a) concentrations compared with those in the bottom third.239 Adjustment for conventional risk factors including LDL cholesterol did not significantly change the association. Moreover, data from the Quebec Cardiovascular Study240 and the Italian Longitudinal Study on Aging241 suggest that, among men, elevated Lp(a) levels interact positively with high LDL cholesterol levels, hypertension, hyperhomocysteinemia and elevated fibrinogen concentrations. In a recent cohort study242 using data from the Nurses' Health Study Initiative — which showed that women in the highest quintile of Lp(a) were twice as likely to develop CVD compared with women in the lowest quintile, independent of other conventional risk factors — no significant interactions with LDL cholesterol, HDL cholesterol or fibrinogen were found. This may be partly explained by the fact that levels of Lp(a) tend to increase with age, more so in women than men,243 which parallels the age-related increase in LDL cholesterol and fibrinogen levels seen in women.
Socioeconomic status
There is a clear socioeconomic gradient in risk of CVD, with those in the lowest socioeconomic strata having the highest risk of cardiovascular events.244,245 Although this gradient exists for both men and women, there is increasing evidence to suggest that there may be an interaction between sex and socioeconomic status in the development of both cardiovascular risk factors and CVD.
Socioeconomic status is a complex construct that is influenced by financial, employment and education experiences. The protective effect of high social standing was convincingly and elegantly demonstrated in the Whitehall study. Marmot and colleagues246 clearly showed that, in a cohort of British Civil servants, those in the lowest social strata were 2.6 times more likely to die from CVD than those in the wealthiest class. This negative relation between CVD and socioeconomic status has been demonstrated consistently in numerous studies throughout the developed world. Recent studies indicate that there may be a gender–socioeconomic status interaction in terms of CVD mortality. Gerward and colleagues247 examined the effect of neighbourhood socioeconomic factors on mortality in the first 28 days after an AMI in a Swedish cohort. They demonstrated that low socioeconomic status and early CVD mortality were most closely associated in men over 75 years of age (p value for trend 0.007). This analysis was limited in that it used ecologic measures of both socioeconomic status and cardiac risk. However, examining the influence of social class on CVD mortality in another large Swedish cohort, Baigi and colleagues248 demonstrated that although labourers have much higher CVD mortality than their white-collar counterparts, female labourers have a CVD mortality risk that is double that of male labourers. Results from the NHANES cohort249 were similar: low-income women had a 61% increase in risk of CVD mortality compared with high-income women. Low income also increased risk of CVD mortality in men, but the elevation (29%) was less striking. This analysis adjusted for several other risk factors that may vary with income, including smoking status, blood pressure, cholesterol level and diabetes status.
Health care access
People with low income do not appear to obtain health care as effectively as the wealthy.250,251 Barriers to health care appear to be larger for poor women than men in both single and multipayer systems. In universal systems in Canada, women are more likely to visit their primary care physician, but are less likely to be referred to specialty care and are more likely to be admitted to hospital.251,252 In private systems, such as those in the United States, women are less likely to be able to afford essential medications. This inability to obtain evidence-based therapy is associated with a 50% increase in the incidence of angina, non-fatal AMI and non-fatal stroke among US women.252
CVD risk factors and health behaviours
Diabetes, obesity, sedentary lifestyle, smoking and hypertension are more prevalent in populations at low socioeconomic levels.253 Lower social class has consistently been found to be associated with lower levels of HDL cholesterol and APO-A1 in both men and women.254 No consistent relation between socioeconomic status and LDL cholesterol has been found. The interaction between socioeconomic status and gender appears to have an impact on specific cardiovascular risk factors. Although low socioeconomic status women are at much greater risk of diabetes mellitus and obesity than men,255,256 the negative relation between smoking behaviour and wealth is more evident in men.
Psychosocial factors
There is increasing awareness of the influence of psychologic and social factors on the development of heart disease.257 In North America, people who experience depressive symptoms are more likely to be women and are more likely to have low income.258 US women who are involuntarily unemployed have been found to have higher blood pressure and higher rates of anginal pain compared with employed women and homemakers. The effect is most striking in African-American women. An unemployed African-American woman is 2.6 times more likely to have CVD compared with an unemployed non-Hispanic white woman.259 Van Lenthe and colleagues260 showed the independent and significant relation between social and financial deprivation and heart disease in the GLOBE study. Even after controlling for the behavioural risk factors smoking, alcohol use, physical inactivity and obesity, material factors such as unemployment, poor housing and crowding were associated with a 25%–80% increase in the incidence of AMI in this Dutch cohort. Wang and colleagues261 suggest that different components of the socioeconomic status construct affect men and women differently. They examined the association of self-reported health with various aspects of socioeconomic status (income, education, social support and connectedness) in a large Japanese cohort (n = 9650). They found that high income was associated with better self-reported health in both men and women. Among those in lower social classes, poor self-reported health was more closely associated with low income in men, but in women, poor self-reported health was more closely associated with social isolation and lack of social support.
Critical analysis of studies
The studies reviewed above include observational cohort studies and cross-sectional assessments. Results of studies specifically focusing on women, on men, or providing sex comparisons were included. Areas not sufficiently addressed by existing studies are highlighted as knowledge gaps.
Why are there sex differences?
Review of the existing literature suggests that sex differences in cardiovascular risk factors are attributable to a combination of biologic and behavioural factors that may be further modified by age, geography and ethnic background. Compared with their male counterparts, adolescent girls and premenopausal women tend to have more favourable risk profiles, not only in terms of blood pressure and serum lipids, but also in terms of emerging cardiovascular risk factors. However, this “sex protection” is much attenuated with age among postmenopausal women. There is a possibility that the evolution of sex differences in risk profiles is at least partly attributable to sex hormones or their receptors. In terms of health behaviour, women tend to be less physically active and are more likely to be obese than men, but smoking rates are higher among adult men than women. Possible reasons for these behavioural differences include child care and household duties limiting physical activity in women, postpartum retention of weight and lower likelihood of smoking because of concerns about its impact during pregnancy. Although lower levels of activity and higher rates of obesity may be offset by better overall cardiovascular risk profiles before menopause, they may contribute to a marked deterioration in risk profile following menopause.
Summary
• Men are more likely to be overweight than women.
• The prevalence of obesity is higher among women, particularly among black women.
• Women tend to be less physically active than men.
• Prior to menopause, women have better cardiovascular risk profiles than men, with lower levels of blood pressure, LDL cholesterol and plasminogen activator inhibitor type-1 and higher levels of HDL cholesterol.
• Following menopause, cardiovascular risk profiles of women and men become more similar.
• Diabetes appears to abrogate the vascular protection afforded to premenopausal women.
• Rates of absolute CVD are higher among men with diabetes than among women with diabetes. However, diabetes accounts for a larger proportion of the CVD that occurs among women than men.
• Smoking rates are higher for men than women.
• The association of APOE phenotype with LDL cholesterol level is significantly greater in postmenopausal women than in premenopausal women or in men.
• Low socioeconomic status has an adverse impact on access to health care and cardiovascular risk profiles.
• Low socioeconomic status is associated with high prevalence of obesity and diabetes in women, but not consistently so among men.
• Women are less likely to be referred for specialty care than men.
Knowledge gap
• What strategies can be employed to optimize detection and treatment of hypertension and dyslipidemia among men and women?
• What are the barriers to improving physical activity levels among women?
• Can the relative risk of CVD among women with diabetes be reduced through optimal diabetes management?
• How can we improve access to health care among women of low socioeconomic status?
Differences in cardiovascular presentation in women and men
Colleen Norris, Kaberi Dasgupta and Susan Kirkland
Increasing evidence suggests that there are sex or gender differences in the presentation and prodromal symptoms of acute coronary syndrome (ACS).262–264 However, the model used to identify the symptoms of ACS continues to be consistently based on data sets in which men are the normative standard.265 Furthermore, this phenomenon, described as the “Yentl syndrome,” has been evidenced by lower use of diagnostic and therapeutic procedures for women and, perhaps more important, a decreased ability to identify female patients at risk for acute coronary events.265 Consequently, if women do in fact experience symptoms that deviate from what is understood as “normal,” the presenting symptoms may not be recognized as prodromal to ACS, resulting in delayed treatment. As well, if women seek attention for the “abnormal” symptoms, they may be misinterpreted by medical personnel, delaying or giving rise to misdiagnosis and lack of treatment typically provided to men.
Search strategy
A comprehensive review of the literature from 1999 to 2005 was undertaken using the following combination of MeSH headings: “myocardial ischemia,” “myocardial infarction,” “unstable angina,” “stable angina” and “presenting symptoms,” “prodromal symptoms” and “gender” and “women.”
Sex differences in symptoms of ACS
Sex differences in anatomic, physiologic, biologic and psychologic characteristics may explain sex differences in symptoms of ACS.264,266 Women have smaller coronary artery lumens and less collateral circulation than men, which may lead to an increase in ischemia, particularly during exertion or stress. From a physiologic perspective, the syndrome X, possibly the result of dysfunctional coronary microvasculature or smooth muscle vasomotor tone, may contribute to the difference in symptoms experienced by women and men. Sex hormones may partly account for symptom differences. For example, diminishing estrogen levels in premenopausal and menopausal women may affect lipid metabolism and the activation of the coagulation cascade and vasoactive mediators. Finally, psychosocial differences between women and men may also explain differences in the experience of symptoms. Depression is 3 times more common in women than men.267 The similarities among symptoms for anxiety, depression and ACS may complicate the diagnostic process.
Sex differences in the diagnosis of ACS
The prevalence of ACS diagnosed in emergency departments is lower for women than men,268 with rates dependent on clinical presentation at admission. The percentage of women diagnosed with ACS can range from 33% to 45%. Most studies addressing sex differences in ACS have focused specifically on AMI.268–270 Framingham data indicate that 69% of women initially present with unstable angina compared with 30% of men.271 As women are less likely to present with AMI, fewer women than men have been studied with respect to ACS presentation. There is a need for studies addressing symptomatology among women with unstable angina, a more common ACS presentation in women.
Sex differences in prodromal symptoms of ACS
Atypical prodromal symptoms in women include fatigue; difficulty breathing, shortness of breath and dyspnea; neck and jaw pain; palpitations; cough; nausea and vomiting; and indigestion. Few studies have addressed prodromal symptoms from a sex perspective. Recently, Bahr and colleagues272 reviewed the “state of the science” about the phenomenon termed “prodromal.” Their search included literature from 1937 to 2000 although “an effort was made to identify the more rigorous studies (in English) from the last 10 years that included randomized prospective trials.” The results highlighted the fact that, although prodromal symptoms appear to play an important role in the evolution of ACS, there is no standard definition of symptoms, nor any consistent pattern in their reporting. More important, of the 28 studies that focused on patients who were diagnosed with AMI, the proportion of women in the study sample, when reported, varied from 11% to 28%, making it impossible to determine whether women and men experienced or described different symptoms. With the exception of the work of McSweeney and colleagues263 whose sample included only women, the studies reported on by Bahr and colleagues did not address differences between women and men in either the presence or proportion of prodromal or acute symptoms reported.
In contrast, in their seminal work on women's prodromal and acute symptoms of AMI, McSweeney and colleagues263 identified a number of important issues that may explain the lack of consistent findings regarding the differences between women and men. The foremost issue was the fact that the tools used to describe the symptoms of ACS are typically closed-ended or structured questions based on retrospective chart reviews from studies conducted primarily on men. Therefore, women are restricted to choices that inaccurately describe their symptoms. In addition, there may be a semantic difference in the definitions of the symptoms themselves. Questions concerning pain “in the back” may be interpreted as lower back pain and may not elicit descriptions of discomfort in the upper back, posterior to the shoulder. The time frame, specifically whether symptoms were prodromal or acute, has not been well described among women. Finally, studies that included only questions on symptoms that occurred during hospital stays and gathered this information retrospectively from hospital records (including the majority of the 28 studies identified by Bahr and colleagues) would have excluded sex differences in symptoms that may have become apparent had patients been queried prospectively.
Having identified these issues, McSweeney and colleagues went on to develop and test the McSweeney Acute and Prodromal Myocardial Infarction Symptom Survey (MAPMISS). In a multicentre study,273 95% of women reported prodromal symptoms before AMI, but only 29.7% reported chest discomfort, a hallmark symptom in men.
Evidence for sex differences in symptoms presentation
Among the 37 studies identified in our search, 8 addressed the diagnosis of ACS;274–281 4 reported on treatment or outcomes;282–285 2 addressed the predictive relation between prodromal symptoms and infarct size;286,287 4 discussed the clinical presentation for other coronary conditions including stent restenosis,288 hemostasis and vascular reactivity,289 calcification290 and nonobstructive coronary disease in women;291 and 1 investigated the presence of “distressed personality.”292 Of the remaining 18 studies, 3 were restricted to women,273,293,294 and 7 observed that women with ACS experience more “atypical” symptoms than men.262–264,266,273,293,295 Ryan and colleagues296 found that patients, namely older adults and women, presenting with atypical symptoms including chest pain in areas other than substernum or left side or no chest pain, often had delayed diagnosis, less-aggressive treatment and higher rates of in-hospital mortality. Similarly, Boccardi and Verde's review265 of gender differences in clinical presentation to the emergency department for chest pain found that women with ACS were older and had a higher prevalence of diabetes and hypertension, longer delays from symptom onset to presentation and higher in-hospital mortality compared with men.
Herein lies the source of the paucity of data concerning sex differences in prodromal and presenting symptoms of ACS. The fact that 69% of women initially presenting with angina compared with 30% of men,264 combined with data that suggest that women with ACS experience more “atypical” symptoms,262–264,266,273,293,295 means that fewer women with ACS are studied, and there is a lack of understanding as to whether the sex–gender differences in prodromal and presenting symptoms of ACS are significant enough to require change in clinical practice.
As shown in reviews,264,297 the data are inconsistent with regard to sex differences in the prodromal and presenting symptoms of ACS. Methodologic issues around the collection of the data, particularly the reliability of retrospective designs that rely on medical records, the understanding of “typical” and “atypical” symptoms of ACS and the presenting diagnostic or inclusion criteria may have significantly altered the results. A greater understanding of the clinical relevance of sex differences in ACS will only be achieved by evaluating both male and female patients with both unstable angina and AMI.
Summary
• Women are more likely than men to present with unstable angina.
• Women experience more atypical symptoms than men.
• Delayed diagnosis and treatment are more likely to occur in women than in men.
• Depression is more likely to occur in women than in men.
Knowledge gap
• A better understanding of typical and atypical symptoms of ACS in women is needed.
• Public health educational programs are needed to raise awareness of factors involved in treating women.
• Research is needed to determine whether gender and sex differences in the symptoms of ACS are significant enough to require a change in clinical practice.
Genetic and sex determinants of hypertension and CVD
Johanne Tremblay, Milan Petrovich and Pavel Hamet
Sex differences have been virtually ignored in genetic studies of hypertension and other CVD, and few studies have focused exclusively on females or have examined the 2 sexes separately. The sexual dichotomy observed in the prevalence of hypertension may be related to genetic factors, including the X and Y chromosomes and the genes that control sex steroids. This section highlights recent studies using genomic approaches to help elucidate the causes of sexual dimorphism in patients and animal models of CVD.
Search strategy
Literature searches were conducted using PubMed with the following keywords: “genomics,” “genetics,” “sex” and “cardiovascular disease,” and “sex” and “genetics.” We also mention our recent studies in rats, in which we were first to search the whole genome for sex differences in the determinants of stress response.
Y chromosome
The Y chromosome is passed intact from father to son. Originally it was thought that most of the genes on the Y chromosome contribute to male differentiation, but it now appears that they may also be responsible for differences in blood pressure and stress responses between males and females.
Several groups have investigated the pathophysiologic mechanisms of the Y chromosome effect. Ely and colleagues298 demonstrated its possible involvement in blood pressure regulation through activation of the sympathetic nervous system. Higher sympathetic nervous system indices, such as plasma norepinephrine and adrenal chromogranin A levels, were observed in male rats, which could result in differences in renal and cardiac norepinephrine turnover. Our studies on stress response have revealed the essential role of the kidney in the Y chromosome effect, as the Y chromosome influences modulation of the response to dietary salt via altered sodium and potassium excretion.299
In humans, Uehara and colleagues300 suggested that a hypertensive father, but not a hypertensive mother, determines blood pressure in male offspring, providing indirect evidence of the importance of the Y chromosome. The impact of the Y chromosome was assessed directly in 2 populations of Caucasian origin301,302 by looking at the association between microsatellite markers located in the centromeric region of the Y chromosome and blood pressure. Some specific markers were significantly associated with diastolic blood pressure and with serum cholesterol levels in Polish males303 and in a Japanese population that was genotyped for an Alu insertion polymorphism.304 Men with the Alu insertion polymorphism had significantly higher HDL levels than those without the variant. Familial data and association studies confirmed that the Y chromosome harbours genes affecting cardiovascular phenotypes. However, such an association was not found in all populations,305 and it is most probable that the genes located within the nonrecombinant Y locus that are closely related to hypertension and other CVD factors may interact with other genes and environmental factors. In addition, the magnitude of the effect differs with ethnic origin.
Only 5% of the Y chromosome participates in meiotic recombination by pairing with the X chromosome; the remaining 95% is not recombined and is male specific. These genes are broadly expressed in various tissues and may thus determine other phenotypic differences between males and females. They also interact with the environment, including risk factors for CVD (such as smoking, higher serum cholesterol, low HDL cholesterol and obesity). The Y chromosome is also suspected of interacting with androgens and their receptors303,306,307 and hormones of the renin-angiotensin-aldosterone system303 in blood pressure regulation.
Although evidence supports the contribution of the Y chromosome to the regulation of blood pressure and other cardiovascular phenotypes in males, no genes on the Y chromosome have been found to contribute directly to hypertension, although confirmation is still required for some candidate genes.308 Genetic heterogeneity (i.e., relevance limited to some families but not to others) at other blood pressure loci tends to obscure the isolated Y chromosome effect.
X chromosome
Whereas the Y chromosome is male specific, the X chromosome is shared by both sexes. Although women have 2 X chromosomes, 1 is inactive. The X chromosome is associated with quantitative trait loci (QTLs) that might play an important role in hypertension and other diseases, such as CVD, cardiovascular malformation, dilated cardiomyopathy, renal diseases and Turner syndrome. QTLs for blood pressure have been mapped on rat chromosomes 10 and X309 and QTLs for hypertensive renal disease, but not for hypertension per se have been mapped on the X chromosome.310,311 Interestingly, the angiotensin type-2 receptor subtype (AT2-R) is located on the X chromosome.312
X-linked disorders
Turner syndrome: Turner syndrome is a result of complete or partial loss of 1 of the 2 X chromosomes in females and is associated with short stature, gonadal dysgenesis, somatic stigmata, cardiovascular and renal anomalies and a large spectrum of other disorders. The increased mortality associated with Turner syndrome is primarily a result of cardiovascular complications. Congenital cardiac anomalies (coarctation of the aorta, bicuspid aortic valve, anomalous venous drainage) are present in 23%–40% of patients. There is an increased risk of aortic dilatation (42%) and dissection, and of ischemic heart disease, and the risk of hypertension is increased 3-fold. In addition, insulin resistance may be present in up to 50% of women with Turner syndrome, and an atherogenic lipid profile favours the development of CAD.313 It has also been shown that systolic, but not diastolic, blood pressure is higher in women with Turner syndrome.314
Dilated cardiomyopathy: Genetic transmission of disease has been identified in a significant proportion of patients with dilated cardiomyopathy. Autosomal dominant transmission is the most frequent mechanism, and several candidate disease loci have been identified by genetic linkage analysis. Three disease genes are currently known: the cardiac actin gene, the desmin gene and the lamin A/C gene. The last-named has recently been found to be responsible for both the autosomal dominant form of dilated cardiomyopathy with subclinical skeletal muscle disease (8% of cases) and the familial form with conduction defects (3% of cases) or the autosomal variant of Emery–Dreifuss muscular dystrophy. The autosomal recessive form of dilated cardiomyopathy accounts for 16% of cases and is characterized by a worse prognosis. An X-linked form of dilated cardiomyopathy manifests in the adult population and is due to mutations in the dystrophin gene. Clinical and experimental evidence suggests that in a large number of cases, dilated cardiomyopathies are diseases of the cytoskeleton.315
Genes of interest on X chromosomes
The renin–angiotensin system plays a pivotal role in blood pressure regulation by influencing salt–water homeostasis and vascular tone. Angiotensin II exerts its effect via 2 receptor types, AT1-R and AT2-R. Both receptor genes are considered good candidates for producing hypertension and CVD.316 A polymorphism in this receptor has been associated with hypertension in women but not in men.317 Moreover, this female-specific association was more pronounced in premenopausal than in postmenopausal women.
Angiotensin-converting enzyme type 2 (ACE2) is another genetic anomaly that may affect hypertension. ACE2, which was discovered recently, is 42% identical to ACE.318 It has been suggested that ACE2 might negatively regulate the activated renin–angiotensin system by diverting the generation of the vasoconstrictor angiotensin II toward the inactive angiotensin 1–9 and vasodilatory angiotensin 1–7 peptides. Competition between ACE2 and ACE for the same substrate could thus serve as a counterbalancing function.319,320 The ACE2 gene maps to a QTL for blood pressure on the X chromosome in hypertensive rats. ACE2 mRNA and protein levels are greatly reduced in the kidney and inversely correlated with elevation in blood pressure, and salt loading was also shown to reduce ACE2 further and raise blood pressure.
Although Benjafield and colleagues321 did not find any significant association between ACE2 polymorphism and essential hypertension, we found a significant association with early onset hypertension in French-Canadian families.322 The impact of the ACE2 variant on hypertension was much stronger in hemizygous males than in heterozygous or homozygous females. We also showed that this variant is associated with obesity. In fact, obesity and smoking appear to be important modifiers of the ACE2 association with predisposition to early onset hypertension.
Autosomal chromosomes and sex differences
Genetic sex differences in the development of hypertension and CVD are not confined to the sex chromosomes. For instance, in the rat, blood pressure is controlled by QTLs affecting different regulatory systems. In a genome scan to search for genetic determinants of blood pressure, we identified specific loci located on different chromosomes for males and females.323,324 Other QTL mapping studies in rats also showed quite different results in males and females.325 Blood pressure QTLs in the female population differed considerably from those previously identified in males, and the same appears to be true in humans. We recently reanalyzed our total genome scans of a cohort of French-Canadian families326 and found sex-specific QTLs for many metabolic phenotypes related to hypertension. Recently, Weiss and colleagues327 expanded this notion into the sex-specific architecture of quantitative traits for various diseases, including CVD and hypertension.
Although sexual specificity of QTL effects can be explained by action of the sex chromosome, hormonal interaction at the transcriptional and post-transcriptional levels represents an alternative possibility that needs to be addressed.
Mitochondrial DNA
Mitochondria have their own genome. No recombination or exchange takes place between mitochondrial DNA (mtDNA), which is transmitted from the mother. This allows tracing of a direct genetic line; if a mutation arises in a woman's mtDNA, every one of her descendants will have that mutation. Mutations of mtDNA can lead to a number of illnesses. Several studies have shown excess maternal transmission of essential hypertension, suggesting possible mitochondrial involvement.328 To assess the contribution of mtDNA to human essential hypertension, Schwartz and colleagues328 carried out systematic, extended screening of hypertensive individuals to identify potentially pathogenic mtDNA mutations. Watson and colleagues329 described a possible mechanism involving energy-driven sodium transport in the renal tubules, which is largely responsible for sodium homeostasis. The energy is provided by numerous mitochondria located in the renal tubular walls. Mutations could lead to aberrant energy production, which, in turn, would lead to sodium retention and ultimately contribute to or cause hypertension. Watson and colleagues' results appear to support the hypothesis that mutations in mtDNA causing renal tubule dysfunction may be partly responsible for the susceptibility to hypertension of African-Americans who have progressed to end-stage renal disease. Moreover, Fukuda and colleagues330 suggest that mtDNA mutations in Japanese diabetic patients are related to the development of diabetes and that these mutations are associated not only with a decrease in insulin secretion but also with advanced diabetic microvascular complications.
Future research
A better understanding of the pathogenetic mechanisms of sexual dimorphism in the development of CVD is clearly needed. The rapid access to vertiginously increasing novel genomic information; the development of powerful tools for fine mapping, including single nucleotide polymorphism microarrays, offering dense coverage of the whole genome; and development of novel genetically designed animal models will help unlock the secrets of sexual dimorphism of CVD, but only if studies are performed in a targeted way in both sexes in humans and animal models. The combination of linkage disequilibrium and functional studies in human and genetically designed rat strains will help identify the genomic determinants implicated in CVD and hypertension. Gender and genoethnic stratification may help decrease the genetic heterogeneity of the studied populations. A major enigma that remains to be unravelled concerns the differences in the contribution of distinct loci in each sex to the same phenotype. Is it all in genes or should we look more carefully at the 99% non-coding material of our genome to find new clues to sex–gender differences in CVD? With the magnificent tools now available, sex-specific therapeutic approaches and, eventually, preventive measures are now foreseeable.
Why are there sex differences?
Sex is a biologic status, determined by sex chromosomes and their interactions with autosomes, X chromosome inactivation, sex hormones and related determinants. It was only recently realized that genes show variation in expression and action in men and women. Sex-specific transcriptional regulation could be due to different growth hormone and sex hormone profiles in the 2 sexes, which can affect the expression of numerous genes, and these genes in turn affect the transcriptome of many tissues.
Gender is in part determined by the above, but also involves social, cultural and educational shaping resulting from societal influences and geoethnic modulation. In this context, the observable traits in humans are a result of both sex and gender influences, even in the presence of a strong genetic component, as the eventual phenotype expression may be modulated differentially in men and women by society. However, many questions remain regarding molecular contributions to sexual dimorphism.
Summary
• The Y chromosome contributes to differences in blood pressure and stress responses between males and females.
• The X chromosome may play an important role in hypertension, cardiovascular malformation, dilated cardiomyopathy, renal disease and Turner syndrome.
• Sex-specific genetic architecture of human traits contributing to CVD is a result of interplay between sex and autosomal chromosomes.
• A polymorphism in the angiotensin II receptor has been associated with hypertension in women but not in men.
• The impact of the ACE2 variant on hypertension is much stronger in males than females, yet the role played by this newly discovered gene in the therapeutic response to antihypertensive agents remains to be determined.
Knowledge gap
• Research addressing sex differences in genetic susceptibility to the development of CVD or CVD outcomes is needed.
• Studies should be performed in a targeted way in both sexes.
• Hormonal interaction at the transcriptional and post-transcriptional levels must be addressed to assess the impact of autosomes on the sexual dimorphism of CVD determinants.
Delivery of cardiac care in women and men
Veena Guru, Jafna Cox, William Amin Ghali, Sherry Grace and Karin H. Humphries
Search strategy
A literature search using MEDLINE was conducted using the keywords “gender,” “women” or “female” in combination with “acute myocardial infarction” and “treatment,” “secondary prevention,” “cardiac catheterization,” “coronary artery bypass surgery” and “percutaneous coronary intervention.” Data from the Canadian Cardiovascular Research Outcomes Team (CCORT) atlas were obtained to elucidate sex-related trends in the delivery of cardiac care in Canada and were aggregated to provide an overview of observed sex differences.
Acute myocardial infarction
Many studies have documented sex differences in the treatment of AMI. Some have found that women present to hospital later after symptom onset, wait longer for initiation of treatment, are less likely to receive treatment and are less likely to be admitted to monitored intensive care settings.331,332 Others suggest that women tend to present when they are older and are more likely to have comorbidities that may make them ineligible for certain therapies.282,333,334 Women are also less likely to receive any type of reperfusion therapy (thrombolysis, angioplasty),335,336 and elderly women in particular have lower rates of thrombolysis compared with men.335 These observations have been documented in other regions of the world337–344 as well as in Canada and the United States (Table 13). However, there are also data suggesting no sex bias in treatment allocation345 and overall rates of reperfusion once they are adjusted for various clinical factors.343,344 Women have also been observed to consume more hospital resources than men.346
Table 13.
Canadian survey data suggest that the delay in seeking treatment may relate to a lack of public awareness of the urgency associated with experiencing “heart attack–like” symptoms.347 This delay has been observed in both men and women, with as many as 50% waiting more than 2 h and 25% waiting more than 5 h.348 The sociodemographic factors that describe those most likely to present late to hospital include female gender, older age, ethnic minority, low income, lower education level and living alone.349 Women are more likely to be concerned about “not troubling others,” whereas men are more likely to have delayed treatment due to no prior knowledge of the option of thrombolysis.350 It has also been suggested that women may be less likely to realize they are having a heart attack for 2 reasons: primarily because their symptoms are more likely to differ from those classically reported and studied in men and secondarily because of sex differences in pain thresholds (i.e., women have been shown to have a higher pain threshold).351 This theory may be supported by the Framingham study observation that the rate of silent or unrecognized AMI is higher in women than men.352
Secondary prevention after acute myocardial infarction
There are no visible sex differences in secondary prevention practice patterns in Canada, at least in terms of medication prescription, such as the use of beta-blockers, statins and ACE inhibitors following admission to hospital for AMI353 (Table 14). This is similar to findings observed in other regions of the world.354–356 In Sweden, no sex-specific differences in access to medical therapy were observed, and no differences in LDL cholesterol levels by sex were documented at 1 year following the implementation of a national quality improvement program targeting secondary prevention following AMI.357 However, this same study demonstrated higher systolic blood pressure values for women suggesting ineffective dosing of antihypertensive drugs relative to men.357
Table 14.
In Canada, older patients are less likely to receive medications for secondary prevention, and this becomes a sex issue as approximately 45% of patients with AMI aged 65 years or older are women.353 This is a significant issue for both sexes and, in fact, some have argued that age is a stronger gradient influencing the bias in secondary prevention than sex.
Sex differences are evident in the lower participation of women in cardiac rehabilitation programs. It is unclear whether this is due to patient-specific issues, such as greater susceptibility of women to depressive symptoms following AMI, which could limit participation in such programs, or to physician factors.358 Physician referral biases have been documented; for example, in one French study, female gender was independently associated with a 56% lower rate of referral to a cardiac rehabilitation program at discharge.355 A recent Canadian study found that after an ischemic coronary event, more women than men reported receiving much less information than they wanted from health professionals in understanding their treatment decisions.359 Whatever the barriers, cardiac rehabilitation is an important part of AMI care that has several physical and psychologic benefits for the elderly and women and, as such, should be more readily available to them.360
Cardiac catheterization
There is a body of literature suggesting that women are less likely to undergo cardiac catheterization after an AMI.361,362 Some have speculated that this may be due to the fact that exercise stress tests are less likely to be positive in women with disease and that the predictive value of these tests is correspondingly lower than in men. When such test characteristics are taken into account, the sex differences disappear.363,364 Nonetheless, sex-based patterns have been noted in the referral of patients for diagnostic testing.365,366 Men are more likely to undergo exercise testing and angiography, whereas women are more likely to receive echocardiography.365 Even after risk adjustment for clinical characteristics, women are still less likely to undergo noninvasive studies and coronary angiography than men (OR for the underuse of angiography within 12 h of an AMI, 1.28; 95% CI 1.15–1.41), with the sex gap widest in the most elderly cohort of patients.342,366 Other research has shown that with changes in techniques over the last few decades, these differences are no longer evident.367
Women admitted to hospital with an AMI are known to have lower rates of severe coronary disease, and this may influence physician referral practices.368 Yet, a recent Dutch study uncovered no sex differences in the extent of coronary disease or in referral patterns for cardiac catheterization.369 Women undergoing stress myocardial perfusion imaging have lower pretest probabilities of coronary disease and, when this is taken into account, there is little evidence for a sex bias in subsequent referral for angiography.370,371 It is important to emphasize, however, that the prognostic implications of a positive result at stress imaging are the same in both men and women.372,373 Finally, as with secondary prevention practices, some argue that age is the major driver for differences in referral for cardiac catheterization after an AMI, not sex.374
Cardiac procedures after acute myocardial infarction
Women in Canada are less likely to undergo percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) after AMI and are more likely to be treated with medical therapy than men (Table 15). This may relate to the fact that women tend to be older than men when presenting with AMI, and referral for revascularization in Canada becomes less likely with advancing age.375 Some reports from the United States have similarly demonstrated lower rates of revascularization for women following AMI.364 Others have found no sex differences in referrals for PCI and CABG, at least not if the cohort examined is limited to those who have already received angiography following AMI.269
Table 15.
In Canada, wait times for revascularization procedures have not been found to differ between sexes.375 However, there is a large age gradient in wait time; elderly women wait much longer than younger women for either PCI or CABG.375
Cardiac procedure rates in all patients with CAD
Studies have repeatedly reported that PCI and CABG rates are higher in men than in women (Table 16) in Canada, the United States376,377 and other regions of the world, including the United Kingdom.378 Reasons commonly given for the lower CABG rates in women include more comorbidity, which augments their operative risk, and smaller coronary arteries, which present greater technical challenges and increase the potential for incomplete revascularization.379,380
Table 16.
A conflicting view has been put forward by investigators who have shown that PCI rates in women are similar to those for men after adjustment for age.368,381 A report from Alberta382 found that apparent sex differences in the rates of revascularization were eliminated once demographic and clinical characteristics were taken into account. Thus, in their view, the observed variation in access reflected appropriate decision-making rather than sex bias. Similarly, other studies have shown that although women were more likely to have PCI compared with CABG, when both procedures were considered there was no sex difference in overall mechanical revascularization rates.383
Critical analysis of studies
The studies reviewed included a combination of retrospective and prospective observational cohort data. There was a paucity of randomized controlled trial evidence regarding sex-related cardiac care delivery.
Why are there sex differences?
The lack of trial evidence for cardiac therapies in women could explain why there appear to be sex differences in their care. Many have attempted to solve this issue through female subgroup analyses of trial data; however, these analyses are often underpowered and subject to bias. As a result, it is no surprise that, internationally, there are numerous reports describing the underutilization of evidence-based cardiac therapies in women. Ongoing surveillance into cardiac care delivery in Canada and elsewhere is needed, as well as, possibly, the development of evidence-based, tailored sex-specific care. We need to develop a better understanding of effective methods of diagnosis of heart disease in women, including sex differences at disease presentation; development of effective treatment, including decision-making specific to women; the dissemination of evidence-based practices specifically targeting those areas neglected for women; and general public awareness of differences in cardiac symptom presentation in women. We hope to pursue these goals in Canada to equalize cardiac care delivery for women.
Summary
• Women present later after onset of symptoms, wait longer for treatment initiation and are less likely to be admitted to monitored intensive care settings than men.
• There are no sex differences in prescription rates for secondary prevention practice.
• Women have lower rates of participation than men in cardiac rehabilitation programs.
• Women are less likely than men to receive PCI or CABG after AMI, and they have lower rates of revascularization.
Knowledge gap
• Determine whether age, comorbidities and clinical presentation are important determinants of access to care.
• Determine whether other factors, such as ethnic origin and socioeconomic status, are important determinants of access to care.
• Implement evidence-based, sex-specific care.
Outcomes of CVD in women and men — clinical trials
Karin H. Humphries, William Amin Ghali, Jafna Cox, Veena Guru and Colleen Norris
Search strategy
Manuscripts were identified by searching MEDLINE between 1982 and June 2005 using the keywords “gender,” “sex,” “women,” “female” and “acute coronary syndrome,” “acute myocardial infarction,” “congestive heart failure,” “atrial fibrillation,” “percutaneous coronary intervention” and “coronary artery bypass graft.” The reference lists from relevant articles were also searched to identify additional studies. Wherever possible, randomized clinical trials, systematic reviews and meta-analyses were identified.
Acute coronary syndromes
Women admitted to hospital for ACS are older than men and have a higher prevalence of diabetes, heart failure and stroke. On admission, women are more likely to have tachycardia, atrioventricular block, pulmonary rales and a high Killip class.384 Women are also more likely to present with non-ST elevation ACS compared with men.385,386 During hospitalization, women are more likely to experience complications such as shock, heart failure, recurrent chest pain, cardiac rupture and stroke.384,387
Several studies have demonstrated sex differences in early mortality (4–6 weeks) after AMI.385,388–394 Crude short-term mortality has been shown to be consistently higher in women, with some studies estimating that it is 0.5–2 times higher than in men. Much of this increase, but not all, is attributable to older age and greater burden of comorbid disease.394,395
CCORT recently completed an evaluation of in-hospital mortality following AMI using administrative data from across Canada. Table 17 provides the sex-specific in-hospital mortality rates from 1997/98 through 1999/2000.396 Consistent with other work, crude mortality was higher in women than men across all age groups.
Table 17.
In contrast, long-term mortality appears to favour women, when adjustments are made for age and differences in baseline conditions.10,392,394 Vaccarino and colleagues10–12 also noted an age–sex interaction in which younger women, but not older women, had higher rates of both long-and short-term mortality compared with men of the same age. These results suggest that younger women with ACS are a particularly high-risk group. At older age, there were no differences in long-term mortality and, in the very oldest group, women had better outcomes than men.
Summary
• Women are more likely than men to present with non-ST elevation ACS.
• Short-term mortality from ACS is higher among women than among men, in part because of their older age at presentation and greater burden of comorbid disease.
• Women have lower long-term mortality from ACS.
• Women < 50 years old with AMI are at particularly high risk of death.
Percutaneous coronary intervention
PCI is the mainstay of treatment for ACS. Although women referred for this procedure have a lower prevalence of prior AMI and left-ventricular dysfunction than men, they have more heart failure that presumably relates to diastolic dysfunction. Of interest, despite the greater burden of comorbid disease, advanced age and severe angina, the extent of angiographic epicardial disease appears to be less than in men.397
In the early days of PCI, registry data demonstrated higher procedural risk and decreased efficacy in women. More recent results from the 1997–98 National Heart, Lung, and Blood Institute Registry suggest that sex differences in outcomes have decreased, and the proportion of women undergoing this procedure has increased to 35%. Despite increased age and more comorbid conditions, including diabetes, hypertension and heart failure, rates of procedural success (95.0% v. 94.2%), in-hospital death (2.2% v. 1.3%), AMI (2.3% v. 3.0%) and emergency CABG (1.3% v. 1.4%) were not different between women and men, respectively. At 1 year, mortality was significantly higher in women than men (6.5% v. 4.3%), as was the combined end point of death–MI–CABG (18.3% v. 14.4%). However, after controlling for baseline differences, sex was not a significant predictor of death, but remained independently associated with the combined end point. This result was driven by the need for subsequent revascularization and may reflect the lower use of stents in women.398
No sex-specific results have been published from the numerous trials comparing bare metal stents with balloon angioplasty. A recent report evaluating in-hospital mortality and target vessel revascularization in patients undergoing elective PCI using 3.0–4.0-mm stents showed no sex differences.399 In trials of drug-eluting stents (DESs), both the SIRIUS and TAXUS IV trials demonstrated similar reductions in restenosis, target vessel revascularization and major adverse cardiac events at 1 year in women and men.400,401 Evidence for long-term outcomes with DESs are lacking, but early data suggest that DESs result in favourable outcomes in small vessels in both women and men.402
In a CCORT evaluation of outcomes after PCI in Canada between 1992/93 and 2000/01, female sex emerged as an independent predictor of in-hospital mortality (OR 1.28; 95% CI 1.15–1.42).403 This result is difficult to interpret as the timeframe of this evaluation covers the balloon angioplasty era for which outcomes in women are known to be poor, as well as the stent era and the start of the DES era, where results have been shown to be better.
Despite evidence of improved outcomes in the contemporary PCI era, vascular complications remain more prevalent among women. Although the development of less aggressive anticoagulation regimens, increased use of weight-adjusted heparin dosing and the use of smaller sheath sizes have reduced vascular complications over time, women still have a 2-fold higher risk of access-site hematomas, bleeding complications requiring transfusion and retroperitoneal bleeds.400
Primary PCI and thrombolysis in ST elevation myocardial infarction
Prompt coronary reperfusion, by PCI or thrombolysis, is the standard of care in ST elevation MI. Clinical trials examining the efficacy of thrombolysis have shown similar benefits in women and men after adjustment for baseline differences, but a greater risk of bleeding in women.385,389–391,393 Hochman and colleagues385 examined outcomes in GUSTO IIb patients by type of coronary syndrome and determined that women with ST elevation had a nonsignificant trend toward greater risk of death or recurrent MI (OR 1.27; 95% CI 0.98–1.63) compared with men, while there was no difference in the non-ST elevation group (OR 0.93; 95% CI 0.72–1.2) and a protective effect in those with unstable angina (OR 0.65; 95% CI 0.49–0.87). A recent meta-analysis of primary PCI v. thrombolysis in patients with ST elevation MI found that primary PCI was significantly better at reducing overall short-term death, non-fatal reinfarction, stroke and the combined end point of death–non-fatal MI–stroke.404 However, sex-specific outcomes were not reported.
Early revascularization in non-ST elevation myocardial infarction
A meta-analysis of early invasive strategy (PCI or CABG) v. conservative treatment in non-ST elevation MI established that primary PCI reduced reinfarction, severe angina and readmission to hospital over a mean follow-up period of 17 months, but with an early mortality hazard that only became a mortality benefit over the long term.405 Again, this meta-analysis did not report sex-specific outcomes; however, 2 of the trials included in the analysis did investigate sex-specific outcomes. The Fragmin and Fast Revascularization during Instability in Coronary artery disease (FRISC II) trial, which enrolled 749 women (30.5%), reported a significant interaction between sex and early invasive strategy; men, but not women, experienced a reduction in death and recurrent AMI.406 In a subsequent analysis of the data from this trial, it was noted that the sex difference in outcome was only in the CABG group (RR 3.74; 95% CI 1.89–7.40), not the PCI group (RR 1.03; 95% CI 0.60–1.80).406
RITA 3, a British Heart Foundation randomized trial of early invasive strategy v. conservative management,407 found a significant interaction between sex and intervention strategy (p = 0.007), with men benefiting from an early invasive approach (OR 0.63; 95% CI 0.41–0.98), but not women (OR 1.79; 95% CI 0.95–3.35).408 In contrast, the TACTICS-TIMI 18 study did not find that women were less likely than men to benefit from an early invasive strategy.409 A cohort study of early revascularization (50% PCI) in 1450 patients with non-ST elevation MI demonstrated that women had comparable short-term outcomes (HR 0.81; 95% CI 0.44–1.48) and better long-term outcomes (HR 0.65; 95% CI 0.42–0.99) compared with men.410 Comparisons of in-hospital and late mortality rates between women and men after primary PCI for AMI are presented in Fig. 10.400

Fig. 10: In-hospital and late mortality rates among women versus men after primary percutaneous coronary intervention for acute myocardial infarction. Note: ACC–NCDR = American College of Cardiology National Cardiovascular Data Registry; CARS = Coumadin Aspirin Reinfarction Study; CADILLAC = Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications; OR = odds ratio; CI = confidence interval. Reproduced with permission from the American Heart Association (Circulation 2005;111:940-53).400
Summary
• After elective PCI, short-term mortality, target vessel revascularization and restenosis rates are similar in women and men.
• Thrombolysis is equally effective in women and men.
• Women have a 2-fold higher risk of bleeding complications than men.
Knowledge gap
• What is the biologic and pathophysiologic basis for less-extensive angiographic disease in women?
• Do women with non-ST elevation MI benefit from an early invasive strategy?
• Is primary PCI superior to thrombolysis in women with ST elevation MI?
Coronary artery bypass graft surgery
The Society of Thoracic Surgeons (STS) database in the United States shows an increase in the proportion of females undergoing CABG from 25.7% in 1990 to 28.7% in 1999.411 In Canada, women constitute 22.3% of CABG patients, and this remained stable between 1992/93 and 2000/01.412
30-day mortality
Sex differences in operative mortality following CABG remain controversial. The issue is difficult to resolve given the lack of women in the few randomized trials that have evaluated the efficacy of CABG compared with medical therapy or PCI.413–415 Observational studies comparing short-term mortality (in-hospital or 30-day) between men and women provide conflicting evidence, with several studies reporting increased mortality in women,379,388,412,416–418 but some demonstrating equivalent outcomes after adjustment for baseline differences.419–423 However, the weight of evidence indicates that short-term mortality is higher in women. The most recent data from the STS National Cardiac Surgery Database for 2002 indicate an operative mortality of 3.54% in women compared with 2.15% in men.424 It is important to note that mortality rates have fallen significantly over time, with a greater decrease in women than men.425
Several theories have been advanced to explain the higher mortality in women, including older age, greater burden of comorbid disease and more urgent revascularization. However, women had better preserved left-ventricular function and less extensive coronary disease.384,388 Smaller coronary arteries in women have also been proposed as a possible explanation for the higher mortality rate,426 but more recent research indicates that the proportion of women with small coronary arteries (< 1.5 mm) is no different than the proportion of men, 57% and 59% respectively.427
Long-term mortality
In contrast, female sex does not appear to confer increased risk of long-term mortality.379,422,428–431 In some studies, women had even better long-term survival than men after adjusting for risk factors.379,420 The reasons for improved long-term, but not short-term, survival are speculative. Survival bias may be a factor or the improved long-term survival may be a reflection of longer life expectancy in women.
Another indication for CABG is to obtain symptom relief and long-term improvement in function and quality of life. Although studies in these areas have not been consistent, the evidence suggests that after CABG women have worse symptom status, poorer physical function, more depression and lower quality of life compared with men.432,433 Depression at the time of CABG has been shown to influence functional outcomes negatively, and this effect is stronger in women than in men.434
Off-pump outcomes
Women may have better outcomes with off-pump surgery.435–438 In women-only cohorts, those undergoing off-pump surgery had better outcomes than women undergoing conventional CABG.436,437 Studies that compared women and men undergoing off-pump surgery demonstrated that female sex was not associated with worse outcomes.435,438 The results of the latter studies should be interpreted with caution as they were retrospective and the sample sizes were small. However, larger, all-female studies are also not definitive, as patient selection cannot be ruled out. Specifically, there is evidence that internal mammary arteries are more commonly used in off-pump patients compared with conventional CABG. Thus, the improved outcomes may be associated with increased use of these arteries.424
Summary
• Although mortality rates after CABG surgery have fallen significantly over time, short-term mortality remains higher among women than among men.
• Women appear to have better long-term survival after CABG surgery.
• Women may have better outcomes with off-pump surgery.
Knowledge gap
• Further assessment of the potential role of vessel size in short-term outcomes is warranted.
• Further evaluation of the benefits of off-pump surgery in women is warranted.
Heart failure
Information on sex differences in heart failure outcomes is limited and not consistent. Among epidemiologic studies, women appear to have better survival rates than men.439,440 In the Framingham study, the 1-year mortality rate was 36% in women compared with 43% in men (HR 0.64; 95% CI 0.54–0.77).439 In NHANES-I, the 1-year mortality rate was 23.8% and 54.4% in women and men, respectively.440 Similarly, in 2 retrospective cohort studies of elderly Medicare patients, women had better survival than men.441,442 Vaccarino and colleagues442 reported lower age-adjusted 6-month mortality in women compared with men (RR 0.81; 95% CI 0.68–0.95), which persisted at 1 year, whereas 30-day mortality did not differ. However, after adjustment for baseline differences, the 6-month mortality risk for women was comparable with that of men (RR 0.90; 95% CI -0.75–1.08). In contrast, women in the Studies of Left Ventricular Dysfunction (SOLVD) registry had a higher 1-year mortality rate (22%) than men (17%).442
Atrial fibrillation
Evidence from the Framingham study suggests that there is no sex difference in mortality rate in patients with atrial fibrillation (OR 1.2; 95% CI 0.98–1.49).32 Analysis of data from the Canadian Registry of Atrial Fibrillation (CARAF), which enrolled patients at the time of their first ECG-documented episode of atrial fibrillation, found that women were, on average, 5 years older than men and more likely to be symptomatic.36 During annual follow-up visits, women were also significantly more likely to report episodes of paroxysmal atrial fibrillation, but progression to permanent atrial fibrillation did not vary by sex.
Outcomes of CVD in women and men — post-admission drug therapy
Karin H. Humphries, William Amin Ghali, Jafna Cox, Veena Guru and Colleen Norris
There is mounting evidence to suggest that women and men respond differently to drug therapy. This sex-based difference may affect the outcomes of patients with CVD.
Search strategy
Manuscripts were identified by searching MEDLINE between 1982 and June 2005, using the keywords “gender,” “sex,” “women,” “female,” “acute myocardial infarction,” “congestive heart failure,” “atrial fibrillation” AND “ACE inhibitors,” “aspirin,” “GPIIb/IIIa inhibitors,” “beta-blockers,” “statins,” “digoxin,” “spironolactone,” “warfarin” and “rate and rhythm control therapy.” The reference lists from relevant articles were also searched to identify additional studies. Wherever possible, randomized clinical trials, systematic reviews and meta-analyses were identified.
Acute myocardial infarction
Practice guidelines based on evidence from randomized clinical trials support the use of ACE inhibitors, ASA, beta-blockers and statins in patients with AMI without contraindications.443–445
ACE inhibitors
A systematic overview of 100 000 patients, randomly assigned to short-term treatment with ACE inhibitors following AMI, failed to demonstrate a statistically significant reduction in risk for women. This may be a reflection of the small number of women enrolled in these trials (22%–27%), rather than lack of effect of ACE inhibition in women.446 In contrast, a meta-analysis of long-term ACE inhibition demonstrated comparable outcomes in men and women with significant reductions in the composite end point (death–heart failure–MI) in men (OR 0.71; 95% CI 0.65–0.77) and women (OR 0.79; 95% CI 0.67–0.93) (pinteraction = 0.34).447
ASA
The Antiplatelet Trialists' Collaboration reviewed 145 trials of ASA use and found that among high-risk patients, women and men benefited equally from the use of ASA in terms of reduction in vascular events.448 ASA use prevented vascular events in 37 out of 100 men, compared with 33 of 100 women. Sex-specific outcomes were not presented in the most recent update from the Antiplatelet Trialists' Collaboration, which reviewed 287 studies of antiplatelet therapy involving 135 000 patients.449 In contrast, ASA use for primary prevention has not been shown to be of benefit in women. In the large Women's Health Study, ASA had a nonsignificant effect on AMI (RR 1.02; 95% CI 0.84–1.25; p = 0.83) and death from cardiovascular causes (RR 0.95; 95% CI 0.74–1.22; p = 0.68), but there was weak evidence that ASA reduced the risk of stroke (RR 0.83; 95% CI 0.69–0.99; p = 0.04).450 In a recent sex-specific meta-analysis of ASA for the primary prevention of cardiovascular events, ASA was shown to reduce the risk of ischemic stroke in women (OR 0.76; 95% CI 0.63–0.93), but not in men (OR 1.00; 95% CI 0.72–1.41).451 Consistent with the Women's Health Study, ASA use in women was not associated with a decreased risk of MI (OR 1.01; 95% CI 0.84–1.21) in contrast with men (OR 0.68; 95% CI 0.54–0.86).451
Platelet glycoprotein IIb/IIIa inhibitors
These agents have been shown to reduce cardiac complications in patients undergoing PCI by blocking the glycoprotein IIb/IIIa receptor, which is the final common pathway leading to platelet aggregation. The literature reports that women have increased platelet function compared with men and, thus, might be expected to benefit more than men from glycoprotein IIb/IIIa inhibition.452 A pooled analysis of 3 large PCI trials — Evaluation of 7E3 for the Prevention of Ischemic Complications (EPIC), Evaluation in Percutaneous Transluminal Coronary Angioplasty to Improve Long-Term Outcome with Abciximab GP IIb/IIIa blockade (EPILOG) and Evaluation of Platelet IIb/IIIa Inhibitor for Stent (EPISTENT) — demonstrated no gender difference in the benefit derived from glycoprotein IIb/IIIa use. Men had a 41% reduction in the composite end point of death–MI–revascularization (p < 0.001) whereas women had a 38% reduction (p = 0.01).453
Three recent meta-analyses of platelet glycoprotein IIb/IIIa inhibitors were identified.454–456 One comparing glycoprotein IIb/IIIa inhibitors with placebo or standard therapy in 3266 patients treated with primary PCI for AMI demonstrated a significant reduction in the 30-day composite end point death–reinfarction–ischemic or urgent target-vessel revascularization (OR 0.54; 95% CI 0.40–0.72). A sex-specific analysis of outcomes was not provided, even though the study population included 26.1% women (n = 852).454 Similarly, a meta-analysis of glycoprotein IIb/IIIa inhibitors use in 27 115 patients with ST elevation MI did not provide sex-specific outcomes, nor did it indicate how many women were included in the evaluation.455 The third analysis by Boersma and colleagues456 evaluated the efficacy of glycoprotein IIb/IIIa inhibitors in patients with ACS who were not routinely scheduled to undergo early revascularization. In this population of 31 402 patients (35% female), glycoprotein IIb/IIIa inhibitors were shown to be efficacious with a 9% 30-day reduction in death or MI (OR 0.91; 95% CI 0.85–0.98). A highly significant sex–treatment interaction was noted (pinteraction < 0.001), with men experiencing benefit (OR 0.81; 95% CI 0.75–0.89), while women were at increased risk of death or MI (OR 1.15; 95% CI 1.01–1.30). The sex difference remained, even after adjusting for baseline differences. However, when patients were stratified by baseline troponin levels, the risk estimates suggested that, in the troponin-positive group, both sexes benefited from treatment, whereas, in the troponin-negative group, neither benefited. The results of this stratified analysis should be interpreted with caution, as 65% of patients were excluded due to missing troponin values.
Beta-blockers
Information on sex differences in outcomes following treatment with beta-blockers is lacking. A meta-analysis of beta-blocker use after AMI by Freemantle and colleagues457 did not provide any sex-specific outcomes; however, 2 observational studies, the Worcester Heart Attack Study458 and the National Cooperative Cardiovascular Project,459 did report sex-specific outcomes. In a community-wide study of 10 374 patients admitted to hospital with confirmed AMI between 1975 and 1999, Silvet and colleagues458 reported beneficial effects of beta-blocker use in both men (OR 0.22; 95% CI 0.18–0.27) and women (OR 0.32; 95% CI 0.26–0.39) in terms of in-hospital mortality. Krumholz and colleagues459 evaluated outcomes in 115 015 patients 65 years and older who survived hospital admission with a confirmed AMI between 1994 and 1995 and reported comparable 1-year mortality in men (RR 0.83; 95% CI 0.76–0.91) and women (RR 0.89; 95% CI 0.81–0.97).
Statins
The first major randomized controlled trial of statins in patients with AMI was the Scandinavian Simvastatin Survival Study (4S).460,461 Women constituted only 19% of the 4444 patients in the trial. The primary end point, mortality, was significantly reduced in men (RR 0.66; 95% CI 0.53–0.80), but not in women (RR 1.12; 95% CI 0.65–1.93). The secondary end point, CHD death–MI–resuscitated cardiac arrest, was significantly reduced in both men (RR 0.66; 95% CI 0.58–0.76) and women (RR 0.65; 95% CI 0.47–0.91). Another major trial in patients with AMI, but average cholesterol levels, was the Cholesterol and Recurrent Events (CARE) trial. Again, women made up only 14% of the 4159 participants, who were randomly chosen to receive pravastatin or placebo.462 In a separate evaluation of outcomes in women, treatment with pravastatin resulted in a 43% (95% CI 4–66) reduction in the primary end point, CAD death and MI, and a 46% (95% CI 22–62) reduction in the combined end point, which also included CABG or PCI.463 In men, the risk reduction for the combined end point was only 20%. A test for interaction between sex and therapy was significant (p = 0.048) suggesting that women had better outcomes than men, but this result should be interpreted with caution, as this was not an a priori hypothesis. The more recent Medical Research Council/British Heart Foundation Heart Protection Study of simvastatin demonstrated comparable efficacy in men and women, who were at high risk of death from CAD.464 In a subgroup analysis by sex, the relative risk reduction in women was 18.9% compared with 21.7% in men, a difference that was not significant (pinteraction = 0.76).
In a recent meta-analysis of 10 randomized controlled trials of statins for primary and secondary prevention, women made up 18.9% of the total sample (n = 23 447).465 The summary relative risk ratios (RRR) were not significantly different for women (RRR 0.77; 95% CI 0.64–0.94) and men (RRR 0.74; 95% CI 0.69–0.79; pinteraction = 0.37). Although the dichotomy of primary and secondary prevention may be somewhat artificial, most of the evidence for the efficacy of statins comes from secondary prevention trials. A systematic review of 6 primary prevention trials concluded that lipid lowering did not reduce total mortality (RR 0.95; 95% CI 0.62–1.46) or CHD events RR 0.87; 95% CI 0.69–1.09) in women.466
Summary
• Evidence of the benefit of short-term treatment with ACE inhibitors in women is lacking; however, long-term treatment reduces the risk of recurrent events.
• ASA use after AMI is equally efficacious in women and men, but ASA use for primary prevention is not of benefit in women.
• There is evidence that primary prevention with ASA may reduce the risk of stroke in women.
• Although clinical trial evidence for use of beta-blockers after AMI in women is lacking, observational trials have demonstrated short-and long-term effectiveness.
• Statin therapy is equally effective in women and men.
Knowledge gap
• The benefits of ASA use in women appear to be limited to secondary prevention. The lack of effectiveness in primary prevention requires further exploration.
Heart failure
Current clinical guidelines recommend therapy with multiple drugs, including ACE inhibitors and beta-blockers to reduce morbidity and mortality, digoxin to reduce readmission to hospital, and the addition of spironolactone in patients with more severe symptoms.467,468
ACE inhibitors
As in other areas of cardiovascular research, women have been underrepresented in heart failure trials. In an overview of 30 randomized trials of ACE inhibitors, neither the reduction in mortality nor the combined end point of mortality and heart failure hospitalizations was significant in women.469 This finding is difficult to interpret, as it may be a reflection of the underenrolment of women in the earlier trials, rather than evidence of less benefit of ACE inhibitors in women with decreased left-ventricular ejection fraction.
The Heart Outcomes Prevention Evaluation (HOPE) trial undertook a preplanned analysis of the effect of ramipril in high-risk women without heart failure and with preserved left-ventricular function. Women constituted 21% of the study cohort, and 37.5% had a prior AMI. Women experienced similar benefits to men. Specifically, women treated with ramipril had significant reductions in the primary end point of MI, stroke or cardiovascular death (RR 0.77; 95% CI 0.62–0.96), as well as fewer strokes (RR 0.64; 95% CI 0.43–0.96) and fewer cardiovascular deaths (RR 0.62; 95% CI 0.44–0.88).470
Beta-blockers
In a post-hoc analysis of the 898 (23%) women enrolled in the Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF) trial of extended-release metoprolol added to optimal therapy with a diuretic and an ACE inhibitor, women on metoprolol experienced a significant (21%) reduction in the primary combined end point of all-cause mortality–all-cause hospitalization.471 Similarly, in a post hoc analysis of Cardiac Insufficiency Bisoprolol Study (CIBIS) II, a study of bisoprolol added to a diuretic and ACE inhibitors, women not only benefited from beta-blockade, but mortality was significantly lower in women compared with men (HR 0.64; 95% CI 0.47–0.86).472 A pooled analysis of 3 trials of beta-blockade — MERIT-HF, CIBIS II, Carvedilol Prospective Randomized Cumulative Survival (COPERNICUS) — revealed a significant female survival advantage (RR 0.69; 95% CI 0.51–0.93).471
Digoxin
In a post hoc analysis of the Digitalis Investigation Group trial of digoxin in patients with heart failure and depressed ventricular systolic function, women had increased risk of all-cause mortality (HR 1.23; 95% CI 1.02–1.47), which was not seen in men assigned to digoxin (HR 0.93; 95% CI 0.85–1.02).473 A recent retrospective analysis of this study determined that excess mortality is seen only when serum concentrations of digoxin exceed 1.2 ng/mL (HR 1.33; 95% CI 1.00–1.76); at concentrations of 0.5–0.9 ng/mL, there was no excess mortality in women (HR 0.8; 95% CI 0.62–1.13).474 A test for interaction between sex, digoxin concentration and mortality was not significant, but this result should be interpreted with caution, as the sample size in this subgroup analysis was small (n = 89 women).
Spironolactone
In the Randomized Aldactone Evaluation Study (RALES), a retrospective analysis by sex revealed that the reduction in risk of death among patients on spironolactone (0.70; 95% CI 0.60–0.82) was similar for men and women.475 Sex-specific relative risks were not provided.
Summary
• The efficacy of ACE inhibitors is uncertain given the small number of women in trials of these drugs and the lack of direct comparisons with men.
• Post hoc analyses suggest that beta-blockers and spironolactone are equally efficacious in women and men.
Knowledge gap
• Most clinical trials have focused on patients with decreased left-ventricular ejection fraction, whereas women are more likely to have preserved ventricular systolic function. Further research is required to evaluate the effectiveness of therapies in this patient group, which comprises predominantly elderly women.
Atrial fibrillation
Warfarin
Undoubtedly the most important advance in atrial fibrillation therapy has been the decreased risk of stroke in patients treated with warfarin. Some evidence suggests that elderly women are less likely to receive warfarin than their male counterparts. According to CARAF, women 75 years of age and older were 54% less likely to receive warfarin, compared with men in this age group.36 This is consistent with results from a British community survey of warfarin use in patients with atrial fibrillation, where the lowest warfarin use was among elderly women.476
In an analysis of pooled data from the 5 major antithrombotic trials, women comprised 26% of the study cohort.477 Female participation ranged from no women in the Stroke Prevention in Nonrheumatic Atrial Fibrillation (SPINAF) trial to 47% women in the Atrial Fibrillation, Aspirin, and Anticoagulation (AFASAK) trial.478,479 In women, warfarin treatment reduced the risk of stroke by 84% (95% CI 55–95), compared with 60% (95% CI 35–76) in men. Although ASA resulted in a significant decreased risk of stroke in men (44%), in women the 23% reduction did not achieve statistical significance.
In CARAF, women on warfarin therapy, predominantly those less than 75 years of age, were 3.35 times more likely than men on warfarin to experience a major bleed.36 Although increased female risk of bleeds has also been described in people undergoing thrombolytic therapy for AMI and oral anticoagulation after hospital admission for deep vein thrombosis,385 increased risk of bleeds was not reported in any of the trials of warfarin use in atrial fibrillation patients. This may reflect the difference in the intensity of anticoagulation monitoring in clinical trials compared with “real world” experience.
Rate and rhythm control therapy
There were no sex differences in response to treatment in the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study, which investigated the efficacy of 2 treatment strategies — rate control v. rhythm control — in high-risk atrial fibrillation patients. Both men (adjusted HR 1.20) and women (adjusted HR 1.30) had a nonsignificant increased risk of death in the rhythm control arm compared with the rate control arm.480
Critical analysis of studies
Wherever possible, we have evaluated randomized controlled trial evidence or meta-analyses based on randomized controlled trials. In some instances, trial evidence was lacking and prospective cohort studies were reviewed. Universally, women were underrepresented in clinical trials and consequently in the meta-analyses, thus limiting the power to detect differences if they do exist. Indeed, the risk of a type-II error is quite large and must be considered when evaluating trials and analyses where no differences were noted.
Where sex differences were noted, these may be due to inadequate adjustment for baseline differences in age and comorbidities, as women enrolled in clinical trials are on average older than men and present with a greater burden of comorbid disease. The most important limitation was the overall lack of sex-specific information in published studies. Although most studies now enrol women, few provide sex-specific outcomes or test for interactions to determine whether sex differences do exist.
Summary
• Warfarin use in women with atrial fibrillation is efficacious for the prevention of stroke, but warfarin is underused in elderly women.
• There is some evidence that women with atrial fibrillation may not benefit from ASA use.
• There appear to be no sex differences in response to rate and rhythm control therapy.
Knowledge gap
• The apparent increased risk of bleeding in women treated with anticoagulants merits further investigation.
Conclusions
CVD affects both women and men, but it is the leading cause of mortality in women. Although many aspects of the disease are similar in women and men, there is a growing body of evidence to support sex and gender dimorphisms in the prevalence, presenting symptoms, management and outcomes of CVD. However, because data are retrieved from retrospective, observational and cross-sectional cohort studies, definitive conclusions about why there are sex differences cannot be drawn. It is imperative that well-designed studies be conducted in which women are adequately represented. These studies must be sufficiently powered to allow statistical inferences and identification of sex-specific outcomes. Understanding how sex and gender differences translate into CVD will help improve the health of women and men.
Footnotes
-
This project is part of GENESIS Interdisciplinary Capacity Enhancement Team, an interdisciplinary enhancement study of the gender and sex determinants of cardiovascular disease funded by the Canadian Institutes of Health Research and the Heart and Stroke Foundation of Canada, grant no. 72565.
This article has been peer reviewed.
Each author has contributed substantially to conception and design, or acquisition of data, or analysis and interpretation of data; drafted the article or revised it critically for important intellectual content and gave final approval of the version to be published.
Competing interests: Dr. Pilote received financial assistance from Merck Frosst to travel to the Canadian Cardiovascular Society in Ottawa in 2006. None declared by the other authors.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.
- 90.
- 91.
- 92.↵
- 93.↵
- 94.
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.
- 130.
- 131.
- 132.
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.
- 143.
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.↵
- 186.↵
- 187.↵
- 188.↵
- 189.↵
- 190.↵
- 191.↵
- 192.↵
- 193.↵
- 194.↵
- 195.↵
- 196.↵
- 197.↵
- 198.↵
- 199.↵
- 200.↵
- 201.↵
- 202.↵
- 203.↵
- 204.↵
- 205.↵
- 206.↵
- 207.↵
- 208.↵
- 209.↵
- 210.↵
- 211.↵
- 212.↵
- 213.↵
- 214.↵
- 215.↵
- 216.↵
- 217.
- 218.↵
- 219.↵
- 220.↵
- 221.↵
- 222.
- 223.↵
- 224.↵
- 225.↵
- 226.↵
- 227.↵
- 228.↵
- 229.↵
- 230.↵
- 231.
- 232.↵
- 233.↵
- 234.↵
- 235.↵
- 236.↵
- 237.↵
- 238.↵
- 239.↵
- 240.↵
- 241.↵
- 242.↵
- 243.↵
- 244.↵
- 245.↵
- 246.↵
- 247.↵
- 248.↵
- 249.↵
- 250.↵
- 251.↵
- 252.↵
- 253.↵
- 254.↵
- 255.↵
- 256.↵
- 257.↵
- 258.↵
- 259.↵
- 260.↵
- 261.↵
- 262.↵
- 263.↵
- 264.↵
- 265.↵
- 266.↵
- 267.↵
- 268.↵
- 269.↵
- 270.↵
- 271.↵
- 272.↵
- 273.↵
- 274.↵
- 275.
- 276.
- 277.
- 278.
- 279.
- 280.
- 281.↵
- 282.↵
- 283.
- 284.
- 285.↵
- 286.↵
- 287.↵
- 288.↵
- 289.↵
- 290.↵
- 291.↵
- 292.↵
- 293.↵
- 294.↵
- 295.↵
- 296.↵
- 297.↵
- 298.↵
- 299.↵
- 300.↵
- 301.↵
- 302.↵
- 303.↵
- 304.↵
- 305.↵
- 306.↵
- 307.↵
- 308.↵
- 309.↵
- 310.↵
- 311.↵
- 312.↵
- 313.↵
- 314.↵
- 315.↵
- 316.↵
- 317.↵
- 318.↵
- 319.↵
- 320.↵
- 321.↵
- 322.↵
- 323.↵
- 324.↵
- 325.↵
- 326.↵
- 327.↵
- 328.↵
- 329.↵
- 330.↵
- 331.↵
- 332.↵
- 333.↵
- 334.↵
- 335.↵
- 336.↵
- 337.↵
- 338.
- 339.
- 340.
- 341.
- 342.↵
- 343.↵
- 344.↵
- 345.↵
- 346.↵
- 347.↵
- 348.↵
- 349.↵
- 350.↵
- 351.↵
- 352.↵
- 353.↵
- 354.↵
- 355.↵
- 356.↵
- 357.↵
- 358.↵
- 359.↵
- 360.↵
- 361.↵
- 362.↵
- 363.↵
- 364.↵
- 365.↵
- 366.↵
- 367.↵
- 368.↵
- 369.↵
- 370.↵
- 371.↵
- 372.↵
- 373.↵
- 374.↵
- 375.↵
- 376.↵
- 377.↵
- 378.↵
- 379.↵
- 380.↵
- 381.↵
- 382.↵
- 383.↵
- 384.↵
- 385.↵
- 386.↵
- 387.↵
- 388.↵
- 389.↵
- 390.
- 391.↵
- 392.↵
- 393.↵
- 394.↵
- 395.↵
- 396.↵
- 397.↵
- 398.↵
- 399.↵
- 400.↵
- 401.↵
- 402.↵
- 403.↵
- 404.↵
- 405.↵
- 406.↵
- 407.↵
- 408.↵
- 409.↵
- 410.↵
- 411.↵
- 412.↵
- 413.↵
- 414.
- 415.↵
- 416.↵
- 417.
- 418.↵
- 419.↵
- 420.↵
- 421.
- 422.↵
- 423.↵
- 424.↵
- 425.↵
- 426.↵
- 427.↵
- 428.↵
- 429.
- 430.
- 431.↵
- 432.↵
- 433.↵
- 434.↵
- 435.↵
- 436.↵
- 437.↵
- 438.↵
- 439.↵
- 440.↵
- 441.↵
- 442.↵
- 443.↵
- 444.
- 445.↵
- 446.↵
- 447.↵
- 448.↵
- 449.↵
- 450.↵
- 451.↵
- 452.↵
- 453.↵
- 454.↵
- 455.↵
- 456.↵
- 457.↵
- 458.↵
- 459.↵
- 460.↵
- 461.↵
- 462.↵
- 463.↵
- 464.↵
- 465.↵
- 466.↵
- 467.↵
- 468.↵
- 469.↵
- 470.↵
- 471.↵
- 472.↵
- 473.↵
- 474.↵
- 475.↵
- 476.↵
- 477.↵
- 478.↵
- 479.↵
- 480.↵
In this issue
{kind=link}
{kind=link}
{kind=link}
{kind=link}
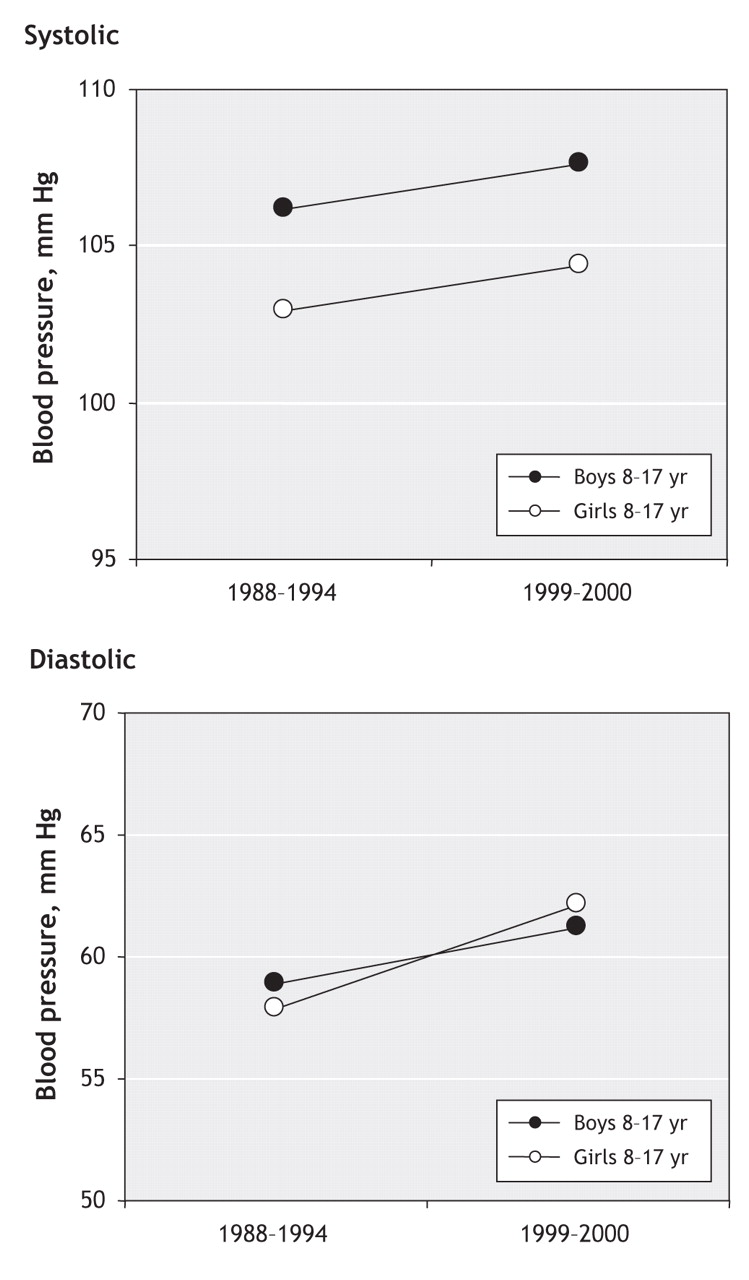{kind=link}
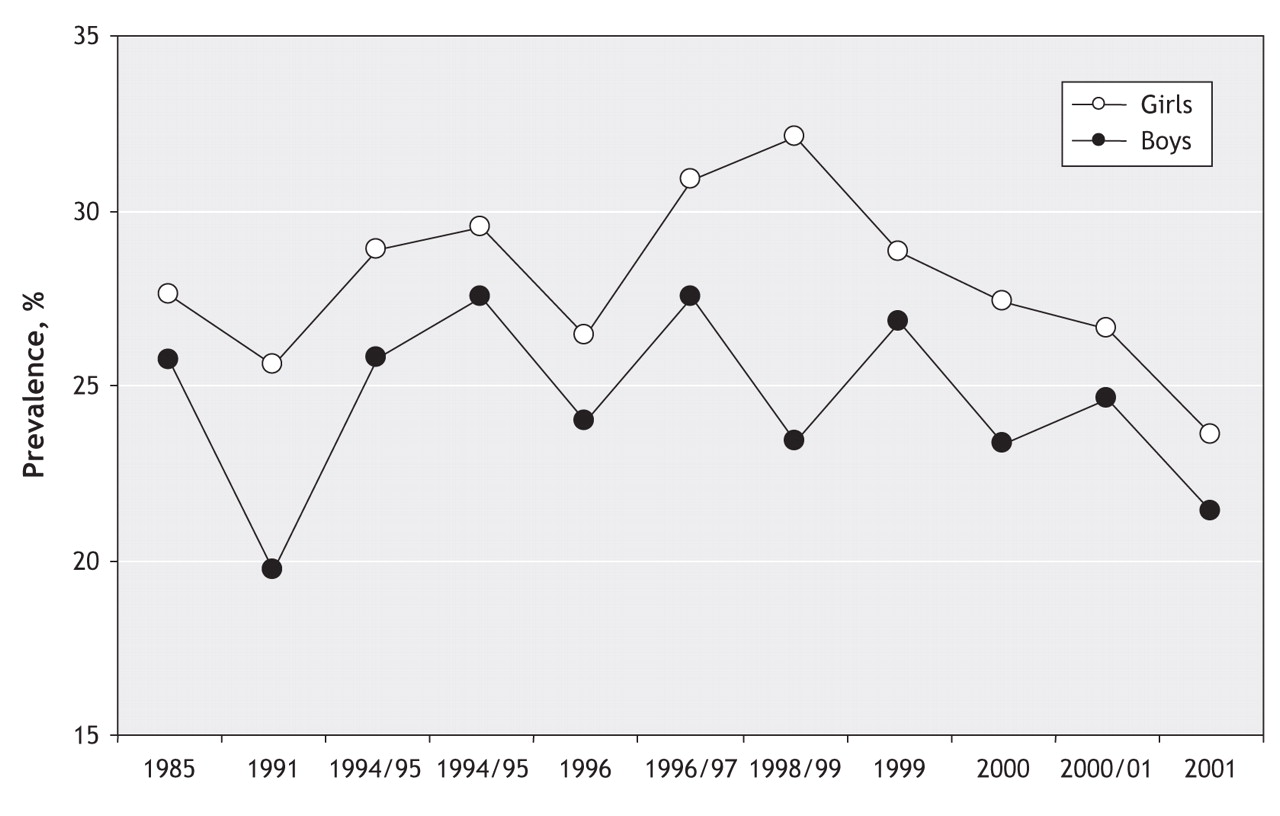{kind=link}
{kind=link}
{kind=link}
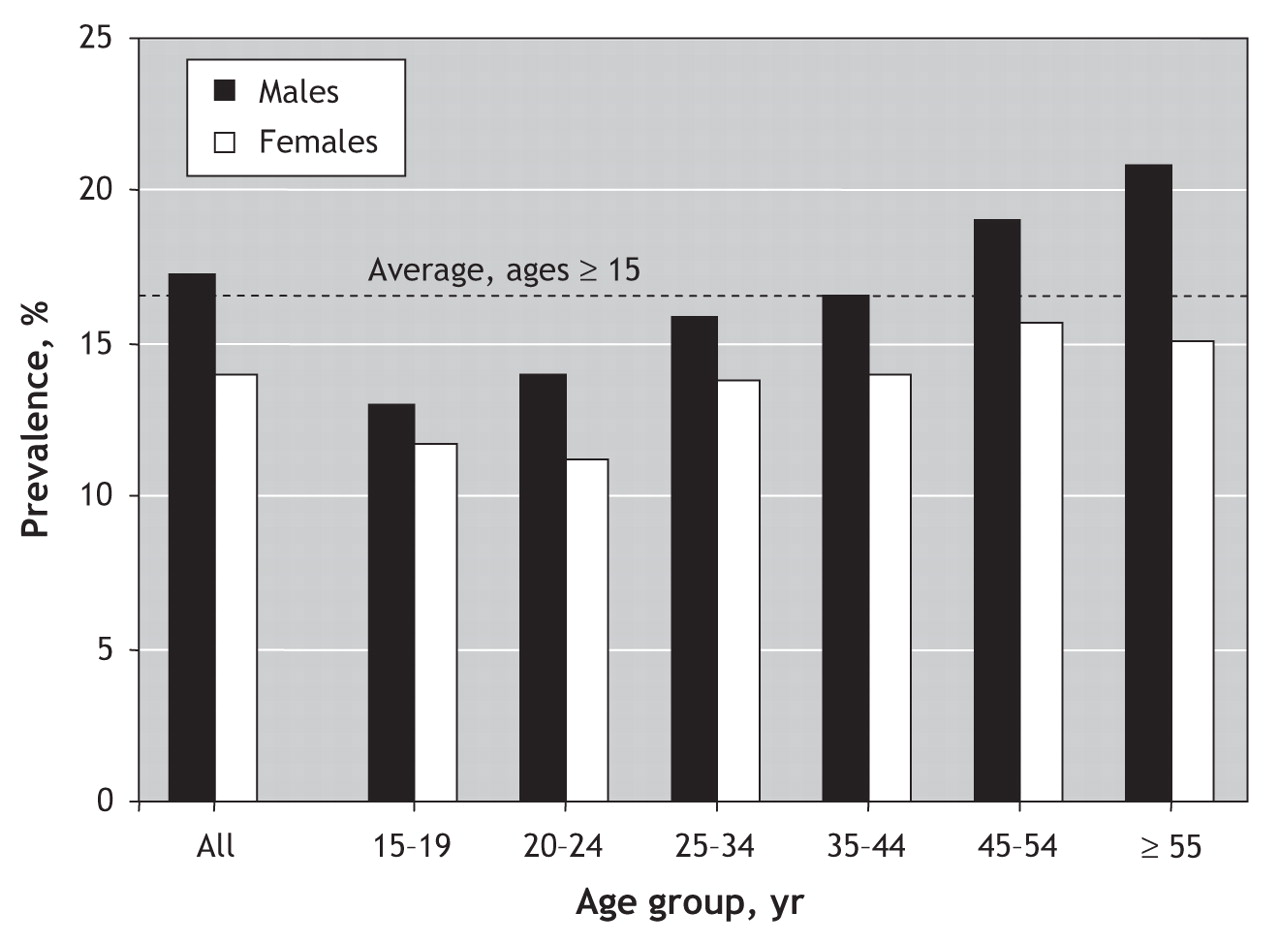{kind=link}
{kind=link}
Article tools






Jump to section
- Article
- Abstract
- Burden of cardiovascular disease in women and men
- Search strategy
- Cardiovascular disease
- Coronary artery disease
- Heart failure
- Atrial fibrillation
- Health-related quality of life
- Summary
- Knowledge gap
- Cardiovascular risk factors in girls and boys
- Search strategy
- Overweight and obesity
- Lipids and insulin resistance
- Blood pressure
- Smoking
- Diet
- Physical activity and sedentary behaviour
- Clustering of behavioural risk factors
- Critical analysis of studies
- Why are there sex differences?
- Cardiovascular risk factors in women and men
- Search strategy
- Overweight and obesity
- Physical activity
- Hypertension
- Diabetes
- Dyslipidemia
- Smoking
- Cardiovascular risk markers
- Socioeconomic status
- Critical analysis of studies
- Why are there sex differences?
- Summary
- Knowledge gap
- Differences in cardiovascular presentation in women and men
- Search strategy
- Sex differences in symptoms of ACS
- Sex differences in the diagnosis of ACS
- Sex differences in prodromal symptoms of ACS
- Evidence for sex differences in symptoms presentation
- Summary
- Knowledge gap
- Genetic and sex determinants of hypertension and CVD
- Search strategy
- Y chromosome
- X chromosome
- Autosomal chromosomes and sex differences
- Mitochondrial DNA
- Future research
- Why are there sex differences?
- Summary
- Knowledge gap
- Delivery of cardiac care in women and men
- Search strategy
- Acute myocardial infarction
- Secondary prevention after acute myocardial infarction
- Cardiac catheterization
- Cardiac procedures after acute myocardial infarction
- Cardiac procedure rates in all patients with CAD
- Critical analysis of studies
- Why are there sex differences?
- Summary
- Knowledge gap
- Outcomes of CVD in women and men — clinical trials
- Search strategy
- Acute coronary syndromes
- Summary
- Percutaneous coronary intervention
- Primary PCI and thrombolysis in ST elevation myocardial infarction
- Early revascularization in non-ST elevation myocardial infarction
- Summary
- Knowledge gap
- Coronary artery bypass graft surgery
- Summary
- Knowledge gap
- Heart failure
- Atrial fibrillation
- Outcomes of CVD in women and men — post-admission drug therapy
- Search strategy
- Acute myocardial infarction
- Heart failure
- Atrial fibrillation
- Critical analysis of studies
- Conclusions
- Footnotes
- REFERENCES
- Figures & Tables
- Responses
- Metrics
Related Articles
Cited By...
- Protocol of the Fit-For-Fertility study: a multicentre randomised controlled trial assessing a lifestyle programme targeting women with obesity and infertility
- Updating the Canadian clinical practice guideline for managing pediatric obesity: a protocol
- Lobesite chez ladulte : ligne directrice de pratique clinique
- Active living environments, physical activity and premature cardiometabolic mortality in Canada: a nationwide cohort study
- Obesity in adults: a clinical practice guideline
- Having a Primary Care Provider is the Strongest Predictor of Successful Follow-up of Participants in a Clinical Trial
- Changing provider behaviour to increase nurse visits for obesity in family practice: the 5As Team randomized controlled trial
- Caregivers readiness for change as a predictor of outcome and attendance in an intervention programme for children and adolescents with obesity: a secondary data analysis
- Canadian Cardiovascular Harmonized National Guidelines Endeavour (C-CHANGE) guideline for the prevention and management of cardiovascular disease in primary care: 2018 update
- Obstructive sleep apnoea and exercise functional capacity: time to move?
- Physical activity assessment and counseling in Quebec family medicine groups
- Different Weight Histories and Risk of Incident Coronary Heart Disease and Stroke: Tehran Lipid and Glucose Study
- Management of acute coronary syndromes: special considerations in women
- Sex disparities in ideal cardiovascular health
- The CHANGE program: Exercise intervention in primary care
- Impact of the 5As Team study on clinical practice in primary care obesity management: a qualitative study
- The Cardiovascular Health in Ambulatory Care Research Team performance indicators for the primary prevention of cardiovascular disease: a modified Delphi panel study
- Collaborative team-based health promotion in a primary care setting: The MOVE program
- Diabetes mellitus among HIV-infected individuals in follow-up care at University of Gondar Hospital, Northwest Ethiopia
- Recent progress in genetics, epigenetics and metagenomics unveils the pathophysiology of human obesity
- Epochs in the depressor/pressor balance of the renin-angiotensin system
- Sex Disparities in Post-Acute Myocardial Infarction Pharmacologic Treatment Initiation and Adherence: Problem for Young Women
- Prevention of overweight and obesity in adult populations: a systematic review
- Canadian Cardiovascular Harmonized National Guidelines Endeavour (C-CHANGE): 2014 update
- Analysis and modelling of cholesterol and high-density lipoprotein cholesterol changes across the range of C-reactive protein levels in clinical practice as an aid to better understanding of inflammation-lipid interactions
- Establishment of Intestinal Microbiota during Early Life: a Longitudinal, Explorative Study of a Large Cohort of Danish Infants
- Obesity in a young child
- The CANHEART health index: a tool for monitoring the cardiovascular health of the Canadian population
- Role of the Waist/Height Ratio in the Cardiometabolic Risk Assessment of Children Classified by Body Mass Index
- Sex Differences in Hospital Mortality in Adults With Congenital Heart Disease: The Impact of Reproductive Health
- Associations of estimated glomerular filtration rate and albuminuria with mortality and renal failure by sex: a meta-analysis
- Childhood social class and adult adiposity and blood-pressure trajectories 36-53 years: gender-specific results from a British birth cohort
- Sex differences in hospital mortality following acute myocardial infarction in China: findings from a study of 45 852 patients in the COMMIT/CCS-2 study
- Cardiac-specific sympathetic activation in men and women with and without heart failure
- Complications associated with adjustable gastric banding for morbid obesity: a surgeons guide
- Cardiovascular Imaging for Assessing Cardiovascular Risk in Asymptomatic Men Versus Women: The Multi-Ethnic Study of Atherosclerosis (MESA)
- 2010 ACCF/AHA Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
- 2010 ACCF/AHA Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the American Society of Echocardiography, American Society of Nuclear Cardiology, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance
- Laparoscopic sleeve gastrectomy: an innovative new tool in the battle against the obesity epidemic in Canada
- Women and Ischemic Heart Disease: Evolving Knowledge
- From the authors:
- Bariatric surgery in patients with bipolar disorder: an emerging issue
- The challenge of obesity treatment: avoiding weight regain
- Gender Differences in Stroke Incidence and Poststroke Disability in the Framingham Heart Study
- Implementing American Heart Association Pediatric and Adult Nutrition Guidelines: A Scientific Statement From the American Heart Association Nutrition Committee of the Council on Nutrition, Physical Activity and Metabolism, Council on Cardiovascular Disease in the Young, Council on Arteriosclerosis, Thrombosis and Vascular Biology, Council on Cardiovascular Nursing, Council on Epidemiology and Prevention, and Council for High Blood Pressure Research
- Gender differences in the long-term outcomes after valve replacement surgery
- Physical Activity and Postmenopausal Breast Cancer: Proposed Biologic Mechanisms and Areas for Future Research
- Euglycemic Hyperinsulinemia Alters the Response to Orthostatic Stress in Older Adults With Type 2 Diabetes
- Depression and Coronary Heart Disease: Recommendations for Screening, Referral, and Treatment: A Science Advisory From the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research: Endorsed by the American Psychiatric Association
- Stroke Incidence, Recurrence, and Case-Fatality in Relation to Socioeconomic Position: A Population-Based Study of Middle-Aged Swedish Men and Women
- Population-Based Prevention of Obesity: The Need for Comprehensive Promotion of Healthful Eating, Physical Activity, and Energy Balance: A Scientific Statement From American Heart Association Council on Epidemiology and Prevention, Interdisciplinary Committee for Prevention (Formerly the Expert Panel on Population and Prevention Science)
- Systematic, Genome-Wide, Sex-Specific Linkage of Cardiovascular Traits in French Canadians
- Visceral adipose tissue and the ratio of visceral to subcutaneous adipose tissue are greater in adults with than in those without spinal cord injury, despite matching waist circumferences
- Characteristics of men and women with diabetes: Observations during patients' initial visit to a diabetes education centre
- Women and coronary disease
- Does Waist Circumference Predict Diabetes and Cardiovascular Disease Beyond Commonly Evaluated Cardiometabolic Risk Factors?
- Long term pharmacotherapy for obesity and overweight: updated meta-analysis
- Pre-eclampsia and increased cardiovascular risk
- Do Women Have Worse Outcome After Stroke Caused by Intracranial Arterial Stenosis?
More in this TOC Section
Similar Articles

