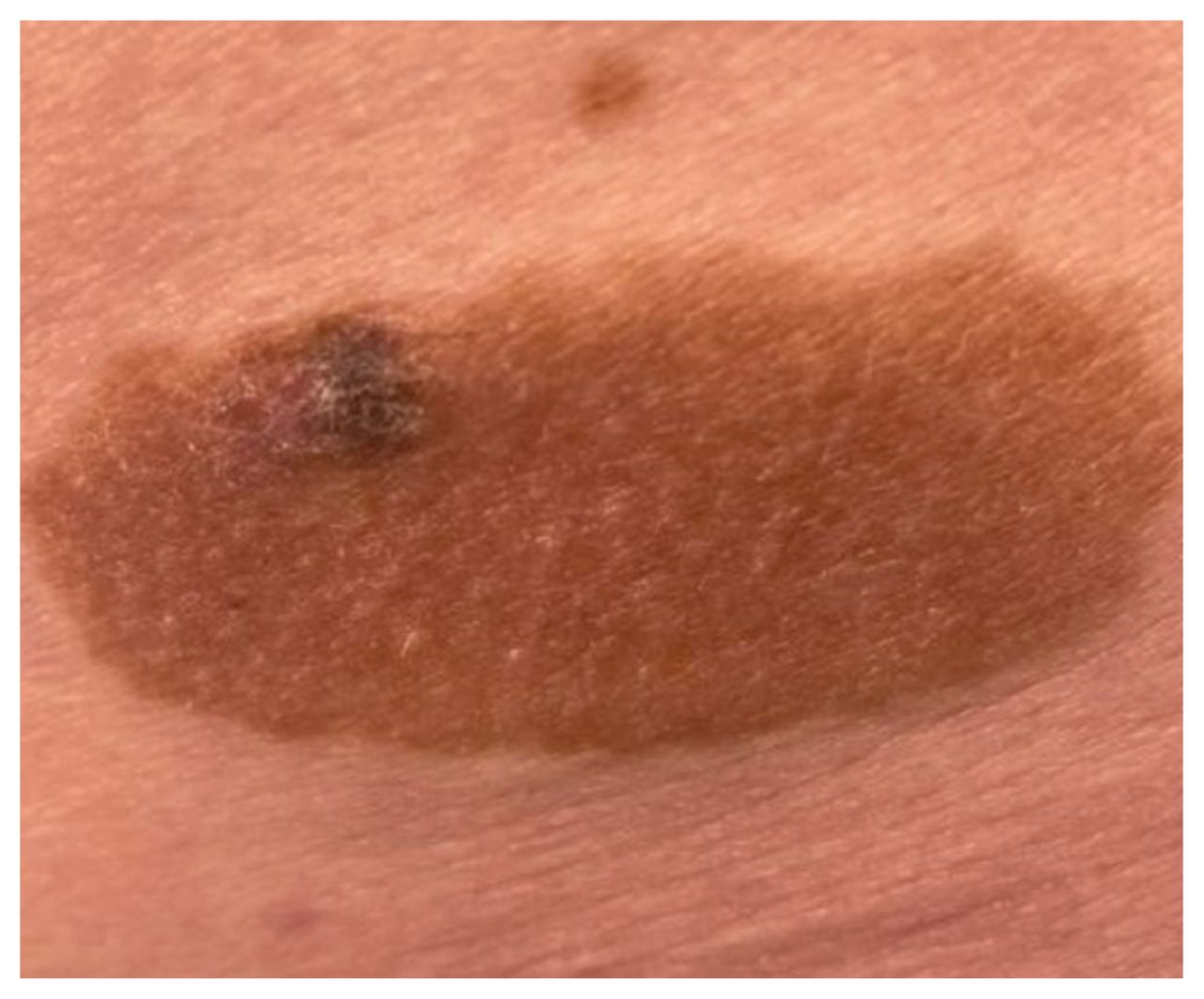
A 69-year-old woman presented to our dermatology clinic with a single congenital melanocytic nevus on her right lower back, measuring 7 × 3 cm, with new-onset pruritus and hyperpigmentation for 1 month (Figure 1). We performed dermoscopy and identified findings concerning for malignancy (i.e., atypical network, irregular pigment dots or globules, irregular blotches, and bluewhite veil), compared with the reticular-globular pattern noted elsewhere within the nevus. We performed a 6-mm punch biopsy, which showed superficial spreading melanoma with a Breslow depth of 0.91 mm. Given the malignant infiltration detected within the papillary dermis without epidermal ulceration, a surgical oncologist performed a wide local excision of the congenital melanocytic nevus and biopsy of the sentinel lymph node. The absence of metastasis indicated localized invasive melanoma (stage T1a N0 M0 in the tumour, node, metastasis staging system). We will continue to monitor her for new skin lesions, lymphadenopathy, hepatosplenomegaly, and subcutaneous nodules at the excision site every 3 months for 2 years, then every 6 months for 2 years, and then annually.
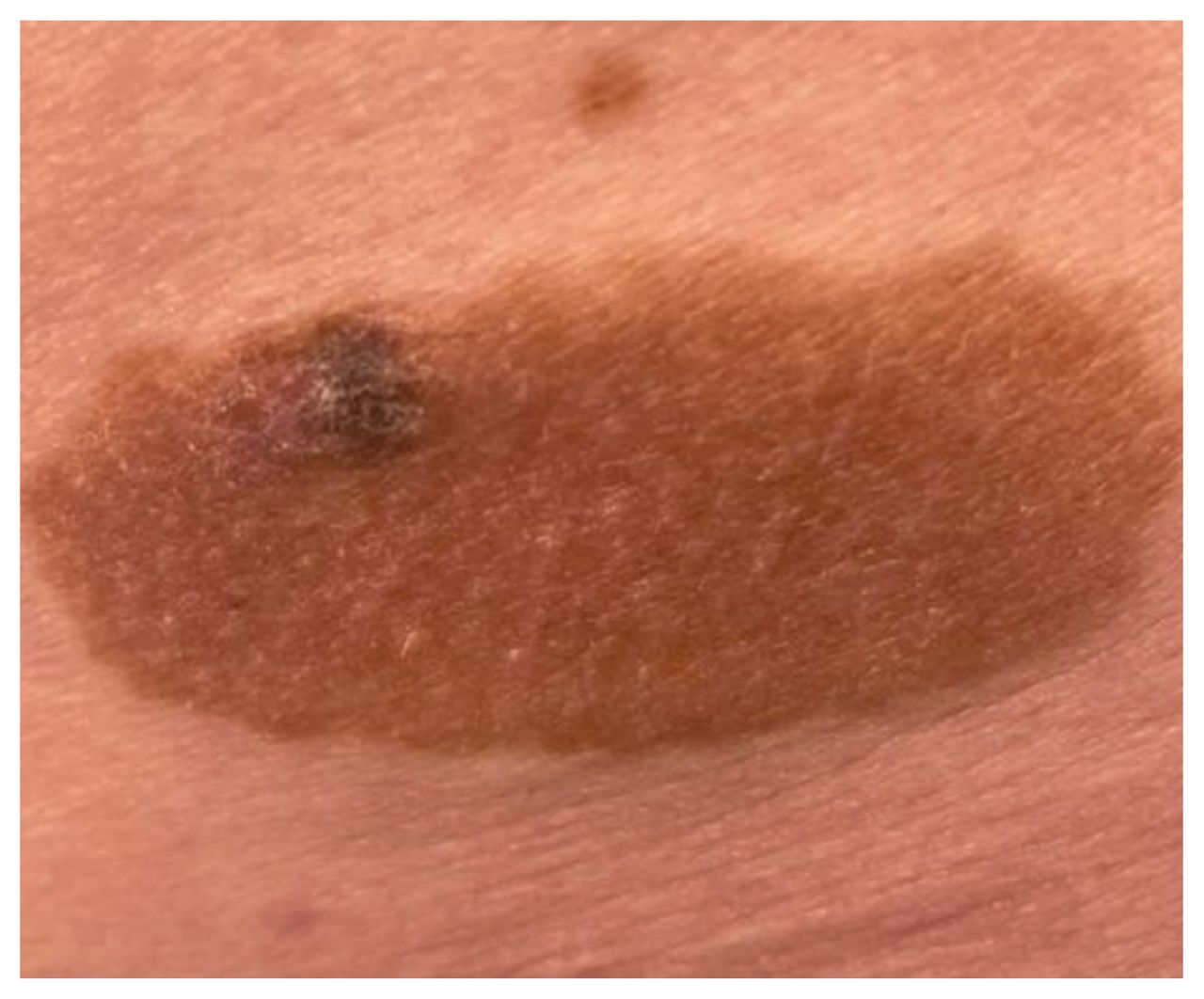
Invasive melanoma of the superficial spreading subtype, arising in a medium-sized congenital melanocytic nevus (7 × 3 cm) on the right lower back of a 69-year-old woman.
Although melanoma in congenital melanocytic nevus is uncommon (1%–5%), delays to diagnosis and treatment increase the risk of morbidity and death.1 Malignant transformation may present with morphologic or colour changes, bleeding, pruritis, or pain, and biopsy should be performed to exclude alternative diagnoses (e.g., seborrheic keratosis).2 Once melanoma is identified, the Breslow thickness should be determined as it is the strongest predictor of metastasis and mortality.2
Most melanomas that arise in congenital melanocytic nevi are of the superficial spreading subtype and occur after puberty (in lesions < 20 cm) or before the age of 5 years (in lesions ≥ 20 cm).3 Prophylactic excision of smaller congenital melanocytic nevi (< 20 cm) solely to avoid malignant disease is unwarranted, given the low risk of malignancy (1%). Similarly, although larger nevi (≥ 20 cm) are more likely to become malignant (5%), excision becomes more impractical with increased size and does not eliminate melanoma risk elsewhere. 1 For early identification and treatment of the development of melanoma, annual full body skin assessments, mole mapping, and dermoscopy, ideally by a dermatologist, are encouraged for patients with a congenital melanocytic nevus of 20 cm or wider in a truncal location, those with multiple nevi (congenital melanocytic nevi or satellite nevi), or those younger than 5 years of age.1–3
Footnotes
Competing interests: Mark Kirchhof reports speaker fees from AbbVie, Amgen, Arcutis, Bausch, Bristol Myers Squibb, Boehringer Ingelheim, Eli Lilly, Incyte, Janssen, Leo, Novartis, Pfizer, Recordati, Sanofi-Genzyme, UCB Biopharma, and advisory board participation with AbbVie, Arcutis, Bausch, BioJamp, Bristol Myers Squibb, Boehringer Ingelheim, Eli Lilly, Incyte, Janssen, Leo, Novartis, Pfizer, Recordati, Sanofi-Genzyme, Therakos, and UCB Biopharma. He is vice-president and head of the membership and stakeholder committee with the Canadian Dermatology Association. All competing interests are outside the submitted work. No other competing interests were declared. This article has been peer reviewed. The authors have obtained patient consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections