Abstract
The primary purpose of this narrative review was to evaluate the current literature and to provide further insight into the role physical inactivity plays in the development of chronic disease and premature death. We confirm that there is irrefutable evidence of the effectiveness of regular physical activity in the primary and secondary prevention of several chronic diseases (e.g., cardiovascular disease, diabetes, cancer, hypertension, obesity, depression and osteoporosis) and premature death. We also reveal that the current Health Canada physical activity guidelines are sufficient to elicit health benefits, especially in previously sedentary people. There appears to be a linear relation between physical activity and health status, such that a further increase in physical activity and fitness will lead to additional improvements in health status.
Physical inactivity is a modifiable risk factor for cardiovascular disease and a widening variety of other chronic diseases, including diabetes mellitus, cancer (colon and breast), obesity, hypertension, bone and joint diseases (osteoporosis and osteoarthritis), and depression.1–14 The prevalence of physical inactivity (among 51% of adult Canadians) is higher than that of all other modifiable risk factors.15 In this article we review the current evidence relating to physical activity in the primary and secondary prevention of premature death from any cause, cardiovascular disease, diabetes, some cancers and osteoporosis. We also discuss the evidence relating to physical fitness and musculoskeletal fitness and briefly describe the independent effects of frequency and intensity of physical activity. (A glossary of terms related to the topic appears in Appendix 1). In a companion paper, to be published in the Mar. 28 issue, we will review how to evaluate the health-related physical fitness and activity levels of patients and will provide exercise recommendations for health.
Several authors have attempted to summarize the evidence in systematic reviews and meta-analyses. These evaluations are often overlapping (reviewing the same evidence). Some of the most commonly cited cohorts have been described in different studies over time as more data accumulate (see Appendix 2, available online at www.cmaj.ca/cgi/content/full/174/6/801/DC1). In this review, we searched the literature using the key words „physical activity,” „health,” „health status,” „fitness,” „exercise,” „chronic disease,” „mortality” and disease-specific terms (e.g., „cardiovascular disease,” „cancer,” „diabetes” and „osteoporosis”). Using our best judgment, we selected individual studies that were frequently included in systematic reviews, consensus statements and meta-analyses and considered them as examples of the best evidence available. We also have included important new findings regarding the relation between physical activity and fitness and all-cause and cardiovascular-related mortality.
All-cause and cardiovascular-related death
Primary prevention
Since the seminal work of Morris and colleagues in the 1950s16,17 and the early work of Paffenbarger and colleagues in the 1970s,18,19 there have been numerous long-term prospective follow-up studies (mainly involving men but more recently women also) that have assessed the relative risk of death from any cause and from specific diseases (e.g., carciovascular disease) associated with physical inactivity.6,20–26
Both men and women who reported increased levels of physical activity and fitness were found to have reductions in relative risk (by about 20%–35%27,28) of death (see Appendix 2, available at www.cmaj.ca/cgi/content/full/174/6/801/DC1). For example, in a study involving healthy middle-aged men and women followed up for 8 years, the lowest quintiles of physical fitness, as measured on an exercise treadmill, were associated with an increased risk of death from any cause compared with the top quintile for fitness (relative risk among men 3.4, 95% confidence interval [CI] 2.0 to 5.8, and among women 4.7, 95% CI 2.2 to 9.8).7
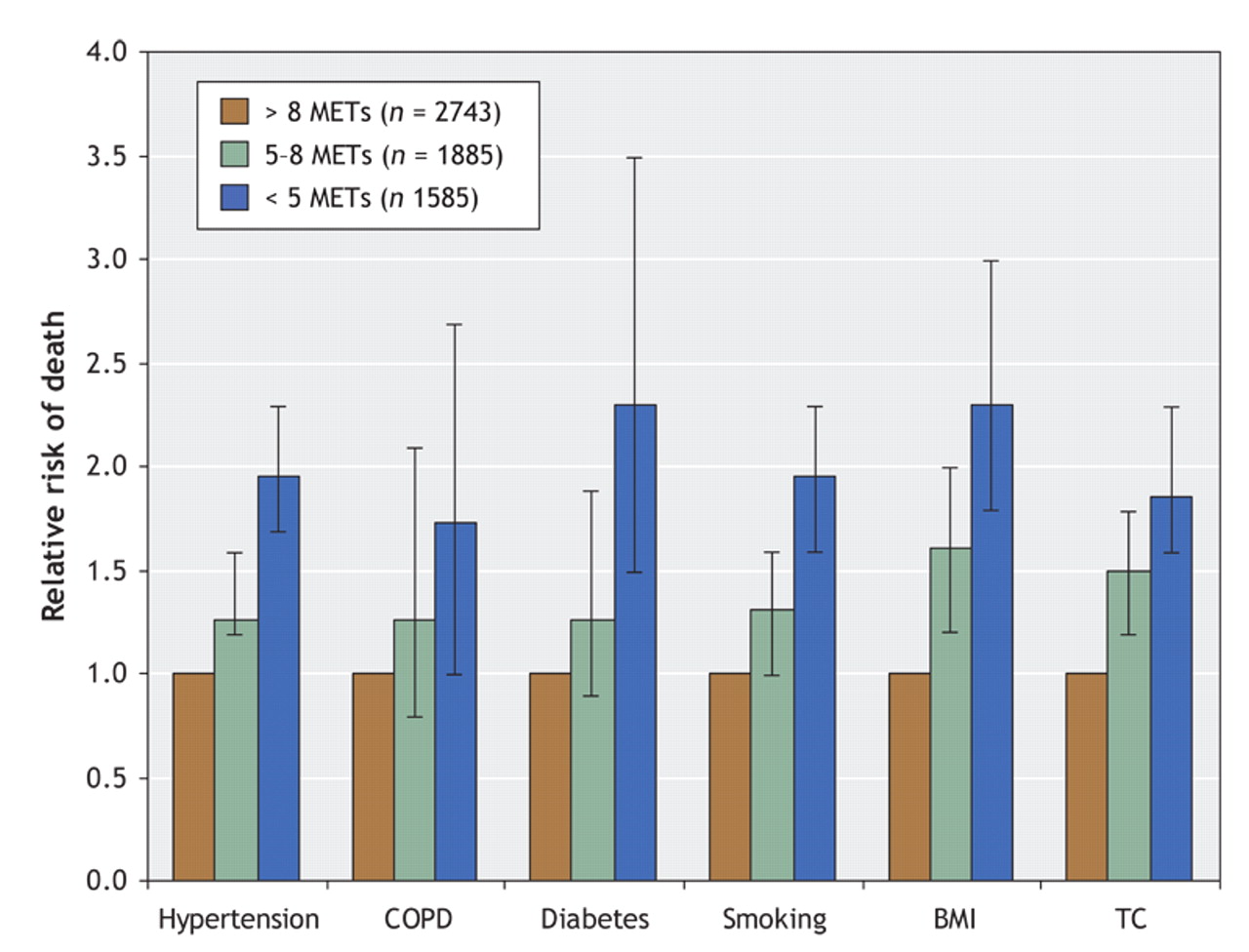
Recent investigations have revealed even greater reductions in the risk of death from any cause and from cardiovascular disease. For instance, being fit or active was associated with a greater than 50% reduction in risk.29 Furthermore, an increase in energy expenditure from physical activity of 1000 kcal (4200 kJ) per week or an increase in physical fitness of 1 MET (metabolic equivalent) was associated with a mortality benefit of about 20%. Physically inactive middle-aged women (engaging in less than 1 hour of exercise per week) experienced a 52% increase in all-cause mortality, a doubling of cardiovascular-related mortality and a 29% increase in cancer-related mortality compared with physically active women.30 These relative risks are similar to those for hypertension, hypercholesterolemia and obesity, and they approach those associated with moderate cigarette smoking. Moreover, it appears that people who are fit yet have other risk factors for cardiovascular disease (see Fig. 1) may be at lower risk of premature death than people who are sedentary with no risk factors for cardiovascular disease.31–33
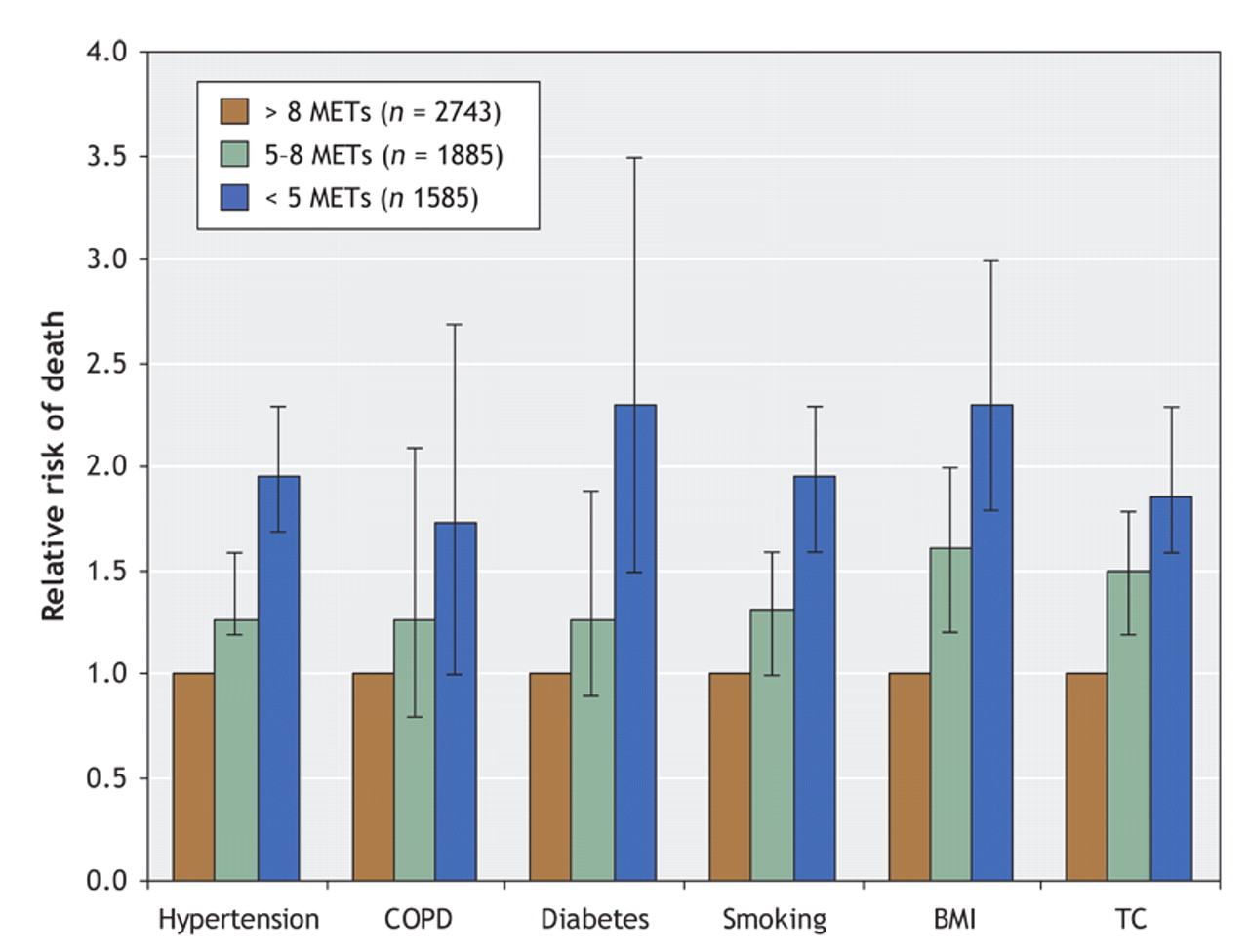
Fig. 1: Relative risks of death from any cause among participants with various risk factors (e.g., history of hypertension, chronic obstructive pulmonary disease [COPD], diabetes, smoking, elevated body mass index [BMI ≥ 30] and high total cholesterol level [TC ≥ 5.70 mmol/L) who achieved an exercise capacity of less than 5 METs (metabolic equivalents) or 5–8 METs, as compared with participants whose exercise capacity was more than 8 METs. Error bars represent 95% confidence intervals. Adapted, with permission, from Myers et al38 (N Engl J Med 2002;346:793-801). Copyright © 2002 Massachusetts Medical Society. All rights reserved.
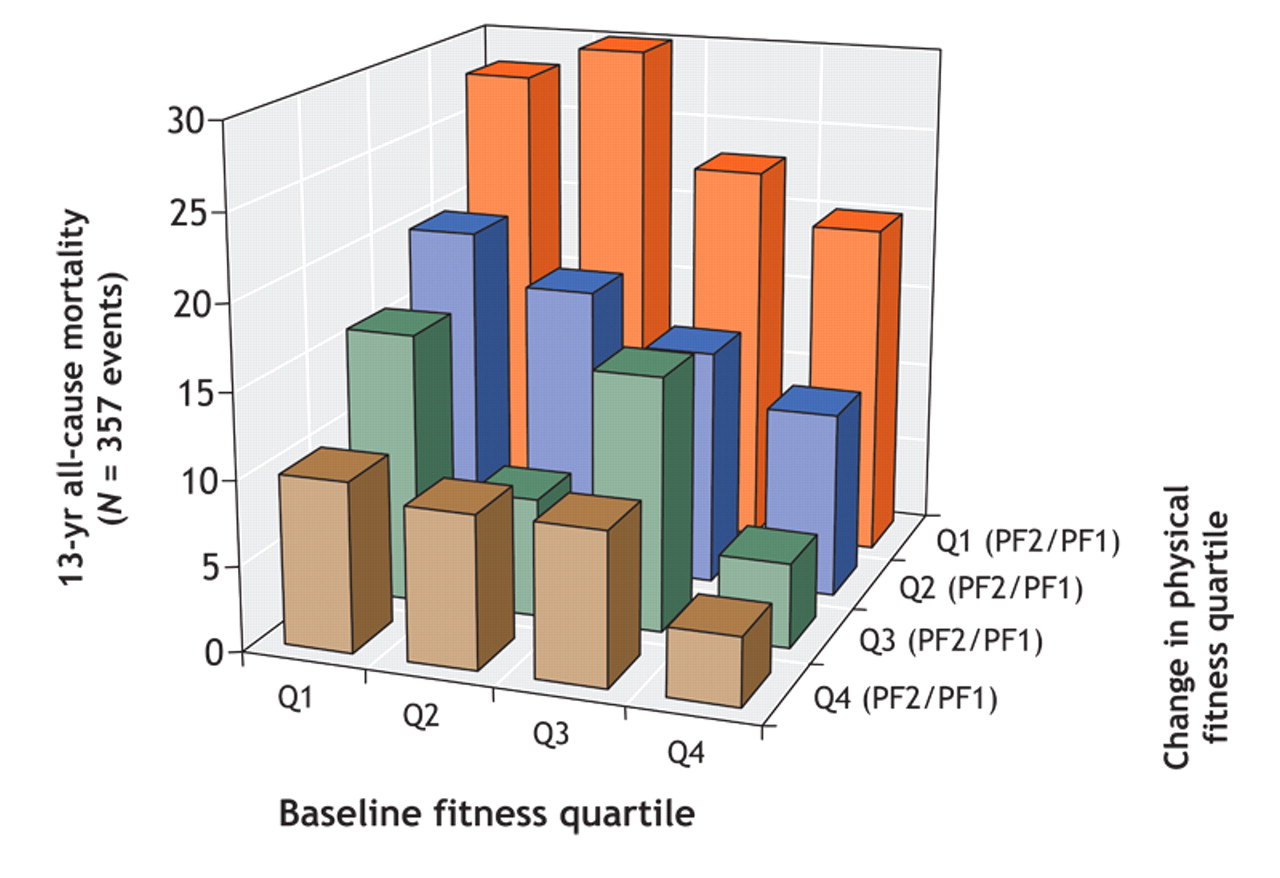
An increase in physical fitness will reduce the risk of premature death, and a decrease in physical fitness will increase the risk.34–37 The effect appears to be graded,34,35 such that even small improvements in physical fitness are associated with a significant reduction in risk (Fig. 2). In one study,35 participants with the highest levels of physical fitness at baseline and who maintained or improved their physical fitness over a prolonged period had the lowest risk of premature death (Fig. 2). Modest enhancements in physical fitness in previously sedentary people have been associated with large improvements in health status.38 For instance, in another study, people who went from unfit to fit over a 5-year period had a reduction of 44% in the relative risk of death compared with people who remained unfit.36
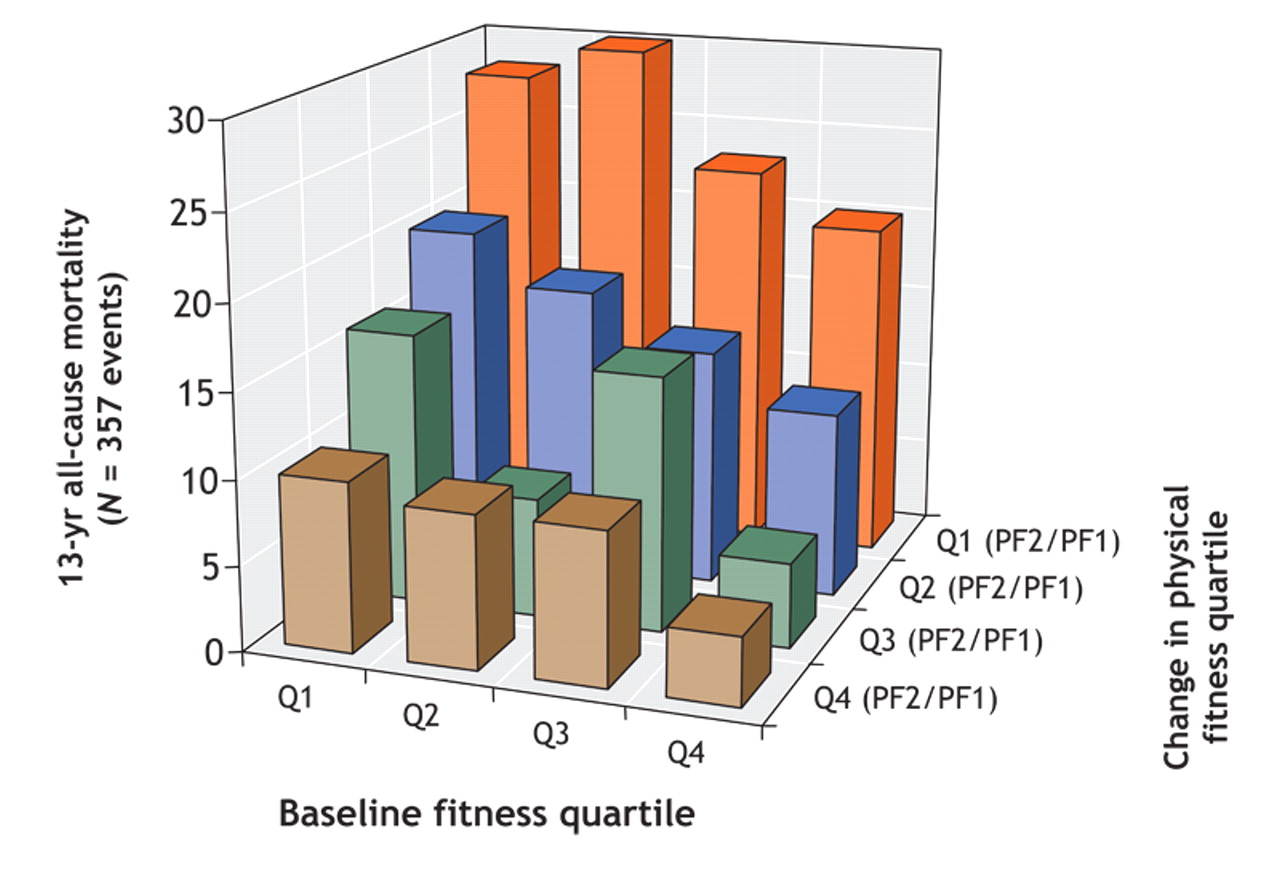
Fig. 2: Relation between changes in physical fitness and changes in mortality over time. Participants were evaluated at baseline (PF1) and again 13 years later (PF2). The ratio of PF2/PF1 × 100 was calculated to evaluate changes in physical fitness over the study period compared with fitness level at baseline. For this figure, participants were grouped according to fitness quartiles (Q1 = least fit, Q4 = most fit) for the baseline evaluation and to quartiles for change in fitness from baseline to 13-year follow-up (Q1 PF2/PF1 = least change, Q4 PF2/PF1 = most change). Adapted, with permission, from Erikssen et al35 (Lancet 1998;352:759-62).
A recent systematic review of the literature regarding primary prevention in women39 revealed that there was a graded inverse relation between physical activity and the risk of cardiovascular-related death, with the most active women having a relative risk of 0.67 (95% CI 0.52 to 0.85) compared with the least active group. These protective effects were seen with as little as 1 hour of walking per week.
In summary, observational studies provide compelling evidence that regular physical activity and a high fitness level are associated with a reduced risk of premature death from any cause and from cardiovascular disease in particular among asymptomatic men and women. Furthermore, a dose– response relation appears to exist, such that people who have the highest levels of physical activity and fitness are at lowest risk of premature death (as discussed later).
Secondary prevention of cardiovascular disease
The benefits of physical activity and fitness extend to patients with established cardiovascular disease.40,41 This is important because, for a long time, rest and physical inactivity had been recommended for patients with heart disease. Unlike studies of primary prevention, many studies of secondary prevention are RCTs (see Appendix 2, available at www.cmaj.ca/cgi/content/full/174/6/801/DC1). Several systematic reviews have clearly shown the importance of engaging in regular exercise to attenuate or reverse the disease process in patients with cardiovascular disease. For instance, a systematic review and meta-analysis of 48 clinical trials5 revealed that, compared with usual care, cardiac rehabilitation significantly reduced the incidence of premature death from any cause and from cardiovascular disease in particular. An energy expenditure of about 1600 kcal (6720 kJ) per week has been found to be effective in halting the progression of coronary artery disease, and an energy expenditure of about 2200 kcal (9240 kJ) per week has been shown to be associated with plaque reduction in patients with heart disease.42,43 Low-intensity exercise training (e.g., exercise at less than 45% of maximum aerobic power) has also been associated with an improvement in health status among patients with cardiovascular disease.44 However, the minimum training intensity recommended for patients with heart disease is generally 45% of heart rate reserve.43
In summary, regular physical activity is clearly effective in the secondary prevention of cardiovascular disease and is effective in attenuating the risk of premature death among men and women.
Diabetes mellitus
Primary prevention
Both aerobic and resistance types of exercise have been shown to be associated with a decreased risk of type 2 diabetes.9,10,45–48 In a large prospective study,46 each increase of 500 kcal (2100 kJ) in energy expenditure per week was associated with a decreased incidence of type 2 diabetes of 6% (relative risk 0.94, 95% CI –0.90 to 0.98)). This benefit was particularly evident among people at high risk of diabetes (i.e., those with a high body mass index), a finding that has been supported by several other investigators.47,49 For instance, among 21 271 male physicians, those who reported weekly physical activity sufficient to cause a sweat had a reduced incidence of type 2 diabetes.47 Moderately intense levels of physical activity (≥ 5.5 METs for at least 40 minutes per week) and of cardiovascular fitness (> 31 mL oxygen per kilogram per minute) have also been shown to be protective against the development of type 2 diabetes in middle-aged men,48 with an even greater effect among those at high risk of diabetes.
Several investigators have reported a reduced incidence of type 2 diabetes among high-risk people (e.g., those who are overweight) after lifestyle interventions.50,51 A review of RCTs on the topic52 concluded that modest weight loss through diet and exercise reduced the incidence of the disease among high-risk people by about 40%–60% over 3–4 years. In one of the RCTs,53 a lifestyle intervention that included moderate physical activity for at least 150 minutes per week was found to be more effective than metformin alone in reducing the incidence of diabetes. It showed that only 7 people would need to be „treated” with the lifestyle intervention to prevent a single case of diabetes over a 3-year period, compared with 14 people given metformin.53
In summary, increasing research supports the importance of regular physical activity for the primary prevention of type 2 diabetes. Further research is warranted to uncover the ideal methods (e.g., resistance v. aerobic training) and intensity levels of exercise.
Secondary prevention
Exercise interventions are also effective in the management of diabetes. One prospective cohort study showed that walking at least 2 hours per week was associated with a reduction in the incidence of premature death of 39%–54% from any cause and of 34%–53% from cardiovascular disease among patients with diabetes.49 Moreover, walking that led to moderate increases in heart and breathing rates was associated with significant reductions in all-cause mortality (hazard rate ratio 0.57, 95% CI 0.41 to 0.80) and cardiovascular-related mortality (hazard rate ratio 0.69, 95% CI 0.43 to 1.09).49 In another cohort study,54 physically inactive men with established type 2 diabetes had a 1.7-fold increased risk of premature death compared with physically active men with type 2 diabetes. This difference has also been observed among people with metabolic syndrome.55
Several clinical trials have been conducted on the topic.56–63 Both aerobic and resistance training have been shown to be of benefit for the control of diabetes; however, resistance training may have greater benefits for glycemic control than aerobic training may have.58 A meta-analysis of 14 controlled trials (11 randomized) revealed that exercise interventions resulted in a small but clinically and statistically significant reduction in glycosylated hemoglobin (0.66%) compared with no exercise intervention;64 in most of the trials, participants in both the exercise and control groups were treated concurrently with oral hypoglycemic agents. This level of change is similar to that observed in studies comparing intensive glucose-lowering therapy with conventional treatments, a change that is known to be associated with a 42% reduction in diabetes-related mortality.64
In summary, exercise interventions for patients with diabetes are beneficial in improving glucose homeostasis. Prospective studies with adequate follow-up show a strong association between exercise and reduced rates of death from any cause and from diabetes in particular. Future research will need to concentrate on examining the effects of dose (intensity and frequency of exercise).
Cancer
Primary prevention
Several seminal reviews have been published regarding the relation between cancer and routine physical activity65–67 (see Appendix 2, available at www.cmaj.ca/cgi/content/full/174/6/801/DC1). Of the available literature (including over 100 epidemiologic studies65),it appears that routine physical activity, whether as part of a job or as a leisure activity, is associated with reductions in the incidence of specific cancers, in particular colon and breast cancer.67–71 A systematic review of epidemiologic studies revealed that moderate physical activity (> 4.5 METs [equivalent to mowing the lawn]) was associated with a greater protective effect than activities of less intensity.65 Physically active men and women exhibited a 30%–40% reduction in the relative risk of colon cancer, and physically active women a 20%–30% reduction in the relative risk of breast cancer compared with their inactive counterparts.65
In summary, there is compelling evidence that routine physical activity is associated with reductions in the incidence of specific cancers, in particular breast and colon cancer.
Secondary prevention
There is a paucity of information regarding the effectiveness of physical activity in preventing death from cancer or from any cause in patients with cancer. An early (5.5-year) follow-up study involving women with breast cancer revealed little association between total recreational physical activity and the risk of death from breast cancer;72 however, the study had some important limitations.73 Two recent follow-up studies involving cancer patients (breast and colon cancer) revealed that increased self-reported physical activity was associated with a decreased recurrence of cancer and risk of death from cancer.74,75 One investigation74 revealed a reduction of 26%–40% in the relative risk of cancer-related death and recurrence of breast cancer among the most active women compared with the least active. Other studies have shown similar associations.75,76 There are ongoing efforts to try to understand the mechanism of this survival effect, including the effects of exercise on the effectiveness of chemotherapy.77 Regular physical activity has also been shown to be associated with an improvement in overall quality of life and health status of patients with cancer.78–82
In summary, regular physical activity appears to confer a health benefit to patients with established cancer. However, further research is warranted to examine its role in the secondary prevention of cancer. In particular, large RCTs evaluating the effectiveness of an exercise intervention are required to fully elucidate the importance of regular physical activity for the health status of patients with cancer.
Osteoporosis
Primary prevention
Weight-bearing exercise, especially resistance exercise, appears to have the greatest effects on bone mineral density. In one review,10 several cross-sectional reports revealed that people who did resistance training had increased bone mineral density compared with those who did not do such training. Furthermore, athletes who engaged in high-impact sports tended to have increased bone mineral density compared with athletes who engaged in low-impact sports.10
Numerous longitudinal studies have examined the effects of exercise training on bone health in children, adolescents, and young, middle-aged and older adults (see relevant reviews83–86 and Appendix 2, available at www.cmaj.ca/cgi/content/full/174/6/801/DC1). Although the numbers of studies and total participants examined are relatively small compared with those in the cardiovascular literature, there is compelling evidence that routine physical activity, especially weight-bearing and impact exercise, prevents bone loss associated with aging. In a meta-analysis of RCTs, exercise training programs were found to prevent or reverse almost 1% of bone loss per year in the lumbar spine and femoral neck in both pre-and postmenopausal women.87 Exercise training appears to significantly reduce the risk and number of falls.88–92
The risk and incidence of fractures is also reduced among active people.93–95 Among 3262 healthy men (mean age 44 years) followed for 21 years,96 intense physical activity at baseline was associated with a reduced incidence of hip fracture (hazard ratio 0.38, 95% CI 0.16 to 0.91). This observation supports findings from an earlier investigation in which fracture rates were lower among people who performed more weight-bearing activities than among sedentary people.97
In summary, routine physical activity appears to be important in preventing loss of bone mineral density and osteoporosis, particularly in postmenopausal women. The benefits clearly outweigh the potential risks, particularly in older people.
Secondary prevention
Preliminary evidence from an RCT indicates that exercise training is effective in improving bone density in older women (75–85 years of age) with low bone mineral density.98 In this 6-month RCT, 98 women were randomly assigned to participate in resistance training (n = 32), agility training (n = 34) or stretching (sham exercise, n = 32). Agility training resulted in a significant increase in cortical bone density by 0.5% (standard error of the mean [SEM] 0.2%) at the tibial shaft, and resistance training resulted in a significant increase in cortical bone density by 1.4% (SEM 0.6%) at the radial shaft; the stretching group experienced losses in cortical bone density.98 Furthermore, a study involving early postmenopausal osteopenic women revealed that a 2-year intensive training program was effective in attenuating the rate of bone loss.99
In summary, preliminary evidence indicates that regular physical activity is an effective secondary preventive strategy for the maintenance of bone health and the fight against osteoporosis.
Physical activity or physical fitness?
Physical fitness refers to a physiologic state of well-being that allows one to meet the demands of daily living or that provides the basis for sport performance, or both. Health-related physical fitness involves the components of physical fitness related to health status, including cardiovascular fitness, musculoskeletal fitness, body composition and metabolism. In large epidemiologic investigations, physical activity and physical fitness are often used interchangeably, with fitness commonly being treated as a more accurate (albeit indirect) measure of physical activity than self-report.100
Physical fitness appears to be similar to physical activity in its relation to morbidity and mortality2,34 but is more strongly predictive of health outcomes than physical activity.6,29,100 Most analyses have shown a reduction of at least 50% in mortality among highly fit people compared with low-fit people (see Appendix 2, available at www.cmaj.ca/cgi/content/full/174/6/801/DC1).29
Nonetheless, both physical activity and fitness are strong predictors of risk of death.29 To obtain accurate estimates of physical activity, many fitness consultants rely on primary (criterion and „gold”) standards for the measurement of energy expenditure, such as direct observation of movement or, in the laboratory, the doubly labelled water technique or indirect calorimetry.101 On a practical basis, however, measures of physical activity and energy expenditure are obtained by using heart rate monitors and motion sensors (pedometers and accelerometers). These devices will be briefly reviewed in the companion article in the Mar. 28 issue.
The assessment of physical fitness is often not feasible or practical in large population-based investigations. Fortunately such studies have consistently shown an inverse gradient of health risk across self-reported physical activity groups. From a public health perspective, Blair and colleagues6 have argued that it is preferable to encourage people to become more physically active rather than to become physically fit, since, as they stated, sedentary people will likely achieve the latter if they do the former.
Musculoskeletal fitness: a paradigm shift
Improvements in indicators of health status can occur as a result of increasing physical activity levels in the absence of changes in aerobic fitness. This is particularly evident in elderly populations, where regular physical activity can lead to reductions in risk factors for chronic disease and disability3,9,10 without markedly changing traditional physiologic performance markers (e.g., cardiac output and oxidative potential).3 Furthermore, routine physical activity can improve musculoskeletal fitness.9,10 There is increasing evidence that enhanced musculoskeletal fitness is associated with an improvement in overall health status and a reduction in the risk of chronic disease and disability.9,10 This research has led to a shift in focus in research related to the health benefits of activities that tax the musculoskeletal system.
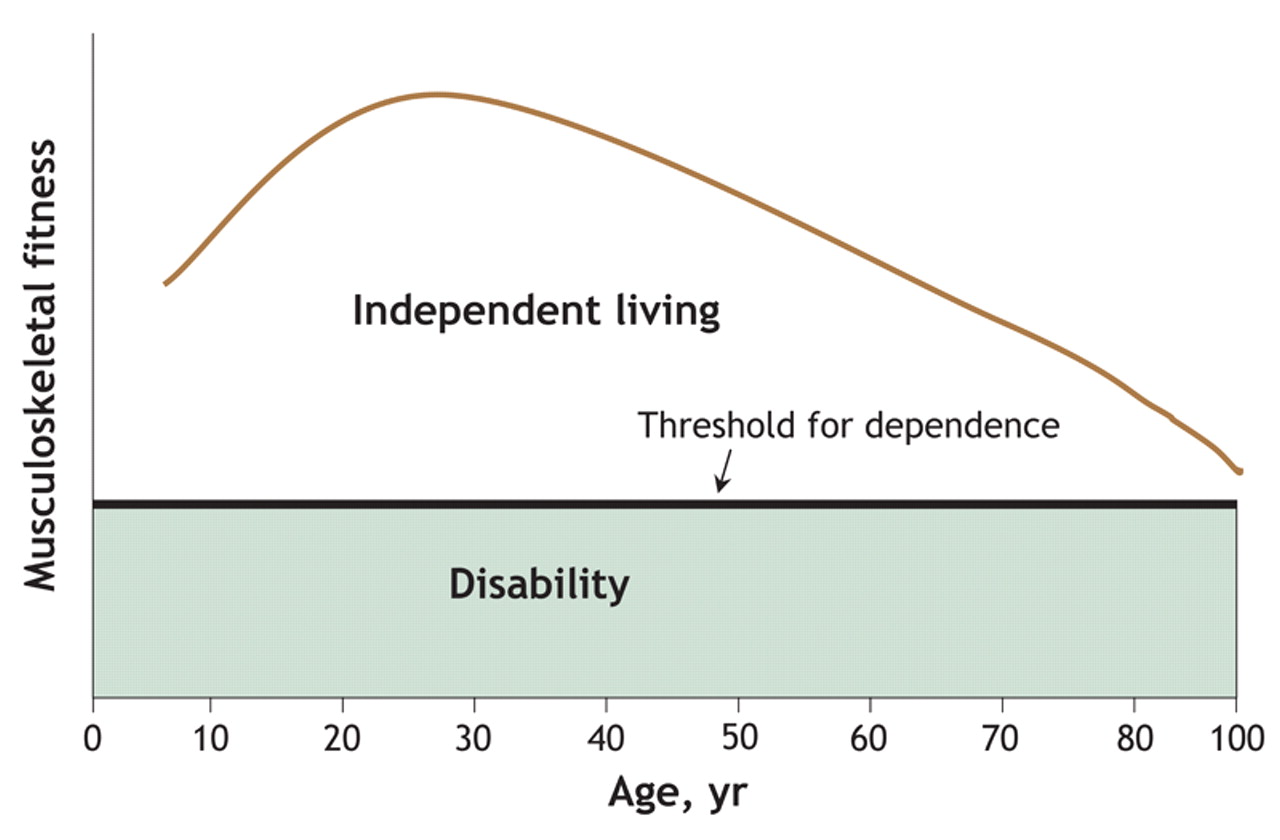
Musculoskeletal fitness appears to be particularly important for elderly people and their ability to maintain functional independence. In fact, many activities of daily living do not require a large aerobic output but depend on one or more of the musculoskeletal fitness components.9,10 As previously stated,10 „Many healthy elderly people may be at or near the functional threshold for dependence, wherein they are in jeopardy of losing the capacity to carry out the activities of daily living. With further worsening of musculoskeletal fitness, an individual may lose the capacity to perform daily activities, such as getting out of a chair or climbing stairs.” This represents a cycle of decline, where reduced musculoskeletal fitness leads to inactivity and further dependence. As illustrated in Fig. 3, improvements in musculoskeletal function have an enormous potential for delaying or eliminating the onset of disability, dependence and chronic disease.9,10 For instance, previous longitudinal investigations have revealed that people with high levels of muscular strength have fewer functional limitations102,103 and lower incidences of chronic diseases such as diabetes, stroke, arthritis, coronary artery disease and pulmonary disorders.103
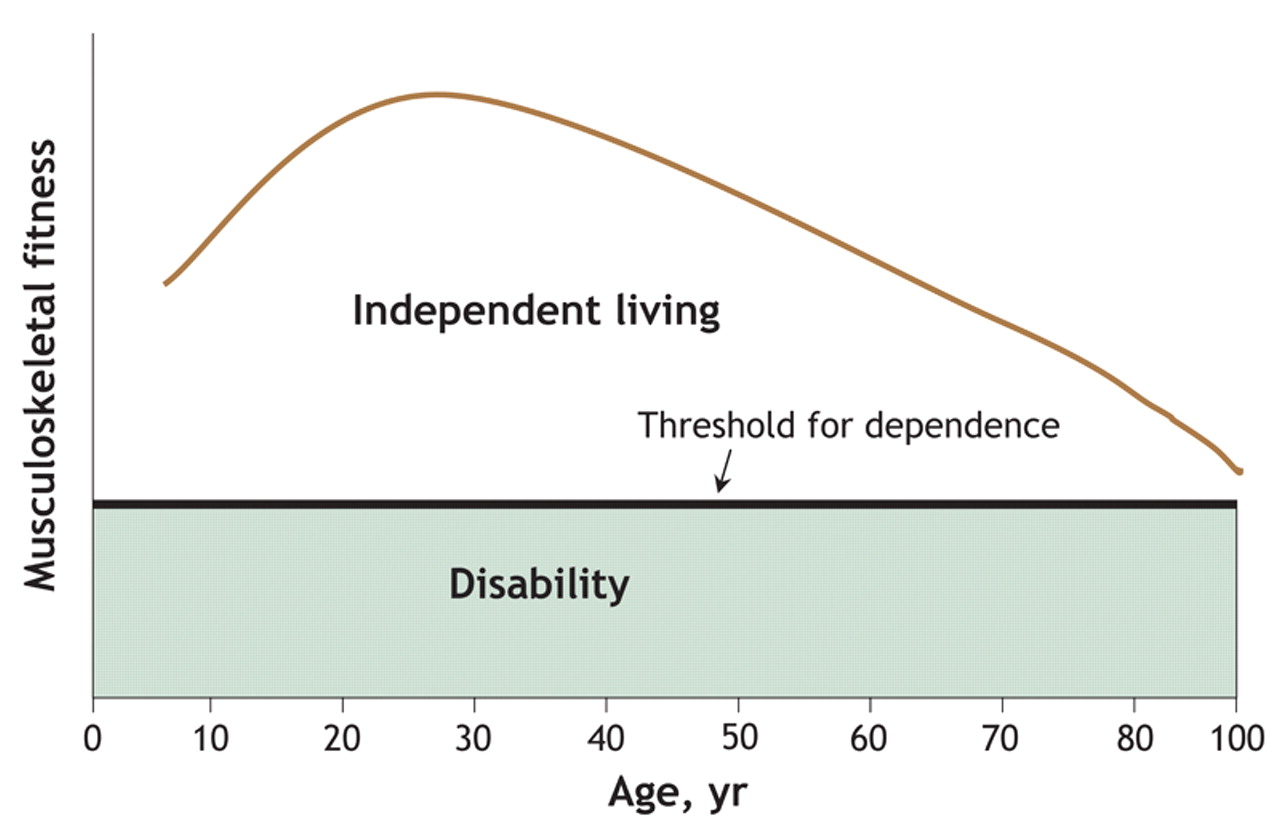
Fig. 3: Theoretical relation between musculoskeletal fitness and independent living across a person's lifespan. As a person ages, his or her musculoskeletal fitness (i.e., muscular strength, muscular endurance, muscular power or flexibility) declines, such that a small impairment may result in disability. Many elderly people currently live near or below the functional threshold for dependence. High levels of (or improvements in) musculoskeletal fitness will enhance the capacity to meet the demands of everyday life and allow a person to maintain functional independence for a greater period.9,10
Two recent systematic reviews9,10 have revealed that enhanced musculoskeletal fitness is positively associated with functional independence, mobility, glucose homeostasis, bone health, psychological well-being and overall quality of life and is negatively associated with the risk of falls, illness and premature death. Interventions that improve musculoskeletal fitness appear to be particularly important for improving the health status of frail elderly people (who have a low musculoskeletal reserve).9,10 This research has revealed clearly the importance of engaging in activities that tax the musculoskeletal system and is supported by findings from a recent epidemiologic investigation.104 This evidence provides direct support for the recent recommendation that resistance training and flexibility exercises be performed at least twice a week to maintain functional status, promote lifelong physical activity and enhance overall quality of life.3,105
How much physical activity is enough?
It is apparent that physical activity is essential in the prevention of chronic disease and premature death.14 However, doubt remains over the optimal „volume” (frequency, duration and intensity of exercise) and the minimum volume for health benefits, in particular the effects of intensity (e.g., moderate v. vigorous) on health status. There is evidence that intensity of physical activity is inversely and linearly associated with mortality.14 Early work by Paffenbarger and associates106 revealed that regular physical activity (expending > 2000 kcal [8400 kJ] per week) was associated with an average increase in life expectancy of 1 to 2 years by the age of 80 and that the benefits were linear even at lower levels of energy expenditure. Subsequent studies have shown that an average energy expenditure of about 1000 kcal (4200 kJ) per week is associated with a 20%–30% reduction in all-cause mortality.14,106,107 Currently, most health and fitness organizations and professionals advocate a minimum volume of exercise that expends 1000 kcal (4200 kJ) per week and acknowledge the added benefits of higher energy expenditures.
Recently, investigators have postulated that even lower levels of weekly energy expenditure may be associated with health benefits.107–109 A volume of exercise that is about half of what is currently recommended may be sufficient,14 particularly for people who are extremely deconditioned or are frail and elderly.6 Future research is required to determine whether expending as little as 500 kcal (2100 kJ) per week offers health benefits. If so, then previously sedentary people may be more likely to engage in physical activity and maintain an active lifestyle.
The dose–response relation between physical activity and health status outlined above generally relates to cardiovascular disease and premature death from any cause. However, the same may hold true for other activity-associated health benefits. For instance, as mentioned earlier, moderately intense levels of exercise (≥ 5.5 METs for at least 40 minutes per week) and of cardiovascular fitness (> 31 mL oxygen per kilogram per minute) are effective preventive strategies against type 2 diabetes.48 In patients with type 2 diabetes, walking more than 2 hours per week has also been shown to reduce the risk of premature death.49
With respect to cancer, a review of the literature revealed that moderate physical activity (> 4.5 METs) for about 30–60 minutes per day had a greater protective effect against colon and breast cancer than activities of low intensity.67 The greatest benefit for reducing the incidence of breast cancer was observed among women who engaged in 7 or more hours of moderate-to-vigorous activity per week.110 Among patients with established cancer, physical activity equivalent to walking 1 or more hours per week was associated with improved survival compared with no exercise.74 The greatest benefit was observed among cancer survivors who performed exercise equivalent to 3–5 hours per week at an average pace.74
With respect to osteoporosis, the dose–response relation of physical activity is less clear. However, osteogenic adaptations appear to be load-dependent and site-specific.9,10,111 Accordingly, physical activities that require impact or significant loading are therefore advocated for optimal bone health. Running distances of up to 15–20 miles (24–32 km) per week has been associated with the accrual or maintenance of bone mineral density, but longer distances may be associated with reduced bone mineral density.112
How does physical activity and fitness lead to improved health outcomes?
Several biological mechanisms may be responsible for the reduction in the risk of chronic disease and premature death associated with routine physical activity. For instance, routine physical activity has been shown to improve body composition (e.g., through reduced abdominal adiposity and improved weight control),9,10,113–116 enhance lipid lipoprotein profiles (e.g., through reduced triglyceride levels, increased high-density lipoprotein [HDL] cholesterol levels and decreased low-density lipoprotein [LDL]-to-HDL ratios),9,10,117–123 improve glucose homeostasis and insulin sensitivity,3,9,10,124–126 reduce blood pressure,127–130 improve autonomic tone,131,132 reduce systemic inflammation;133 decrease blood coagulation,134,135 improve coronary blood flow,136 augment cardiac function137,138 and enhance endothelial function.139–142 Chronic inflammation, as indicated by elevated circulating levels of inflammatory mediators such as C-reactive protein, has been shown to be strongly associated with most of the chronic diseases whose prevention has benefited from exercise. Recent RCTs have shown that exercise training may cause marked reductions in C-reactive protein levels.143 Each of these factors may explain directly or indirectly the reduced incidence of chronic disease and premature death among people who engage in routine physical activity.
Routine physical activity is also associated with improved psychological well-being (e.g., through reduced stress, anxiety and depression9,10,144). Psychological well-being is particularly important for the prevention and management of cardiovascular disease, but it also has important implications for the prevention and management of other chronic diseases such as diabetes, osteoporosis, hypertension, obesity, cancer and depression.
Changes in endothelial function may be a particularly important adaptation to routine physical activity. Endothelial dysfunction has been observed with aging, smoking and multiple chronic disease states, including coronary artery disease, congestive heart failure, stroke, type 2 diabetes, hypertension, hypercholesterolemia and obesity.116 Regular aerobic activity has been found to improve vascular function in adults independent of changes in other risk factors142,145 and has been said to result in a shear-stress–mediated improvement in endothelial function,116 which confers a health benefit to a number of disease states.146
Although most research into the mechanisms of how physical activity and fitness improve health outcomes has dealt with the relation between cardiovascular disease and physical activity, researchers have also evaluated the primary mechanisms responsible for decreases in the risk and severity of individual disease states. In fact, despite the adaptations that are of global benefit for multiple disease states, physical activity also results in specific adaptations that affect individual disease states. For instance, in type 2 diabetes, adaptations that affect glucose homeostasis are of great importance. As reviewed by Ivy,147 a series of changes (independent of changes in body mass64) occur as a result of regular physical activity, including increased glycogen synthase148 and hexokinase activity,149 increased GLUT-4 protein and mRNA expression,148,150 and improved muscle capillary density (resulting in improved glucose delivery to the muscle).149 A series of mechanisms may explain the 46% reduction in cancer rates observed with regular physical activity,66 including reductions in fat stores,66 increased energy expenditure offsetting a high-fat diet,66 activity-related changes in sex hormone levels, immune function, insulin and insulin-like growth factors, free-radical generation,151 and direct effects on the tumour.151
The majority of proposed mechanisms have been discussed in the context of chronic adaptations brought about by routine physical activity. However, researchers have recently examined the importance of acute changes in risk factors for chronic disease.152 An excellent review of the topic by Thompson and colleagues revealed that acute, dynamic exercise may result in transient changes in the form of reductions in triglyceride levels, increases in HDL cholesterol level, decreases in blood pressure (for 12–16 hours), reductions in insulin resistance and improvements in glucose control.152 These acute changes indicate the important role individual exercise sessions have on health status.
Summary
There is incontrovertible evidence that regular physical activity contributes to the primary and secondary prevention of several chronic diseases and is associated with a reduced risk of premature death. There appears to be a graded linear relation between the volume of physical activity and health status, such that the most physically active people are at the lowest risk. However, the greatest improvements in health status are seen when people who are least fit become physically active. The current activity guidelines promoted by Health Canada appear to be sufficient to reduce health risk. People who engage in exercise at levels above those recommended in the guidelines are likely to gain further health benefits. Health promotion programs should target people of all ages, since the risk of chronic disease starts in childhood and increases with age.
In the next issue, we will review how to evaluate the health-related physical fitness and activity levels of patients and will provide exercise recommendations for health.
Footnotes
-
This article has been peer reviewed.
Contributors: Darren Warburton was responsible for the conception of the review and the writing of the manuscript. Shannon Bredin provided assistance with the writing of the manuscript and background research. Crystal Whitney Nicol provided assistance with background research. All of the authors critically reviewed the article for intellectual content and approved the final version.
Acknowledgements: This research was supported by the Michael Smith Foundation for Health Research, the Canadian Institutes of Health Research, the Canada Foundation for Innovation and the BC Knowledge Development Fund.
Competing interests: None declared.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.
- 5.↵
- 6.↵
- 7.↵
- 8.
- 9.↵
- 10.↵
- 11.
- 12.
- 13.
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.
- 58.↵
- 59.
- 60.
- 61.
- 62.
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.
- 69.
- 70.
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.
- 80.
- 81.
- 82.↵
- 83.↵
- 84.
- 85.
- 86.↵
- 87.↵
- 88.↵
- 89.
- 90.
- 91.
- 92.↵
- 93.↵
- 94.
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.
- 115.
- 116.↵
- 117.↵
- 118.
- 119.
- 120.
- 121.
- 122.
- 123.↵
- 124.↵
- 125.
- 126.↵
- 127.↵
- 128.
- 129.
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.
- 141.
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
- Article
- Abstract
- All-cause and cardiovascular-related death
- Diabetes mellitus
- Cancer
- Osteoporosis
- Physical activity or physical fitness?
- Musculoskeletal fitness: a paradigm shift
- How much physical activity is enough?
- How does physical activity and fitness lead to improved health outcomes?
- Summary
- Appendix 1
- Footnotes
- REFERENCES
- Figures & Tables
- Related Content
- Responses
- Metrics
Related Articles
Cited By...
- Intensity of habitual physical activity and maintenance of normal blood pressure - findings from the SUN longitudinal cohort study
- Walking for transport and all-cause mortality: a prospective cohort study of Australian community-dwelling older adults
- TENDINopathy Severity assessment-Achilles (TENDINS-A): evaluation of reliability and validity in accordance with COSMIN recommendations
- Accelerometer-derived physical activity and the risk of death, heart failure, and stroke in patients with atrial fibrillation: a prospective study from UK Biobank
- Evidence based exercise prescriptions in primary care
- Processed food intake assortativity in the personal networks of East European older adults
- Intervention of muscle-building and antifrailty exercise combined with Baduanjin for frailty of different functional levels: study protocol for a randomised controlled trial
- Free to Run: the organisation that uses physical activity to develop female leaders in regions of conflict
- TENDINopathy Severity assessment - Achilles (TENDINS-A): Evaluation of reliability and validity in accordance with COSMIN recommendations
- Association between engagement in cultural activities and use of general practitioner consultations: 7-year follow-up of adults from the HUNT study, Norway.
- Effects of adding exercise to usual care in patients with either hypertension, type 2 diabetes or cardiovascular disease: a systematic review with meta-analysis and trial sequential analysis
- Association between engagement in exercise training and peak cardiac biomarker concentrations following ST-elevation myocardial infarction
- Effects of physical, psychosocial and dual-career loads on injuries and illnesses among elite handball players: protocol of prospective cohort study
- Developing and Validating a Novel Tool to Enhance Functional Status Assessment: The Tennessee Functional Status Questionnaire (TFSQ)
- Promotion of physical activity-related health competence using digital workplace-based health promotion: protocol for a controlled before-and-after study
- Qualitative study of practices and attitudes towards physical activity among prediabetic men and women in urban and rural Malawi
- Proinflammatory Diets and Risk of ESKD in US Adults with CKD
- Socioeconomic inequalities in sport participation: pattern per sport and time trends
- Subjective and Objective Assessment of Physical Activity in Older Adults: Results from Berlin Aging Study II
- Physical activity and its correlates in people with cystic fibrosis: a systematic review
- Association between chronic pain and physical activity in a Swiss population-based cohort: a cross-sectional study
- Physical activity in patients with amyotrophic lateral sclerosis: Prevalence, patients perspectives and relation to the motor performance
- Video-based smartphone app ('VIDEA bewegt) for physical activity support in German adults: a single-armed observational study
- Urine proteomics as a non-invasive approach to monitor exertional rhabdomyolysis during military training
- The potential for bike riding across entire cities: quantifying spatial variation in interest in bike riding
- Social isolation is linked to classical risk factors of Alzheimers disease-related dementias
- Association of physical activity with risk of hepatobiliary diseases in China: a prospective cohort study of 0.5 million people
- Participation and Psychological Capital in Adults With Parkinson's Disease: Mediation Analysis Based on the International Classification of Functioning, Disability, and Health
- Indicators of response to exercise training: a systematic review and meta-analysis
- Comparing the genetic and environmental architecture of blood count, blood biochemistry and urine biochemistry biological ages with machine learning
- Using deep learning to predict age from liver and pancreas magnetic resonance images allows the identification of genetic and non-genetic factors associated with abdominal aging
- An ecosystem service perspective on urban nature, physical activity, and health
- Intraocular pressure fluctuation during resistance exercise
- Promoting physical activity in primary care: a systematic review and meta-analysis
- Analyzing the multidimensionality of biological aging with the tools of deep learning across diverse image-based and physiological indicators yields robust age predictors
- Using financial incentives to increase physical activity among employees as a strategy of workplace health promotion: protocol for a systematic review
- Muscle Strength Explains the Protective Effect of Physical Activity against COVID-19 Hospitalization among Adults aged 50 Years and Older
- Performing arts as a health resource? An umbrella review of the health impacts of music and dance participation
- Female and male US Olympic athletes live 5 years longer than their general population counterparts: a study of 8124 former US Olympians
- Exploring health in the UK Biobank: associations with sociodemographic characteristics, psychosocial factors, lifestyle and environmental exposures
- Body muscle gain and markers of cardiovascular disease susceptibility in young adulthood: prospective cohort study
- Associations between physical activity and trimethylamine N-oxide in those at risk of type 2 diabetes
- Educational differentials in domain specific physical activity by ethnicity, age, and gender: findings from over 44,000 participants in The UK Household Longitudinal Study (2013-2015)
- Barriers and Motivators to Engage in Exercise for Persons with Parkinsons Disease
- Interventions promoting physical activity among adults and children in the six Gulf Cooperation Council countries: protocol for a systematic review
- Is running associated with a lower risk of all-cause, cardiovascular and cancer mortality, and is the more the better? A systematic review and meta-analysis
- Changes in work factors and concurrent changes in leisure time physical activity: a 12-year longitudinal analysis
- Video-based smartphone app ('VIDEA bewegt) for physical activity support in German adults: a study protocol for a single-armed observational study
- Educational differentials in key domains of physical activity by ethnicity, age and sex: a cross-sectional study of over 40 000 participants in the UK household longitudinal study (2013-2015)
- Cost-effectiveness of telephone coaching for physically inactive ambulatory care hospital patients: economic evaluation alongside the Healthy4U randomised controlled trial
- Combined health risks of cigarette smoking and low levels of physical activity: a prospective cohort study in England with 12-year follow-up
- Effects of low-intensity and high-intensity cycling with diesel exhaust exposure on soluble P-selectin, E-selectin, I-CAM-1, VCAM-1 and complete blood count
- Exercise opens a temporal window for enhanced cognitive improvement from subsequent physical activity
- Relationship between cricket participation, health and well-being: scoping review protocol
- Effects of photobiomodulation therapy combined to static magnetic field in strength training and detraining in humans: protocol for a randomised placebo-controlled trial
- Relationship of sociodemographic and lifestyle factors and diet habits with metabolic syndrome (MetS) in a multi-ethnic Asian population
- Health economic assessment of a scenario to promote bicycling as active transport in Stockholm, Sweden
- Mechanical regulation of bone homeostasis through p130Cas-mediated alleviation of NF-{kappa}B activity
- Cost-effectiveness of physical activity interventions in adolescents: model development and illustration using two exemplar interventions
- Process evaluation of team-based care in people aged >65 years with type 2 diabetes mellitus
- Associations between physical activity and cataract treated surgically in patients with diabetes: findings from the 45 and Up Study
- How does exercise treatment compare with antihypertensive medications? A network meta-analysis of 391 randomised controlled trials assessing exercise and medication effects on systolic blood pressure
- Comparison of physical activity and body composition in a cohort of children born extremely preterm or with extremely low birth weight to matched term-born controls: a follow-up study
- Effects of different types and frequencies of physical activity on the homeostatic model assessment of insulin resistance
- Improvement of motor performance in children with cerebral palsy treated with exoskeleton robotic training: A retrospective explorative analysis
- Footballs InfluencE on Lifelong health and Dementia risk (FIELD): protocol for a retrospective cohort study of former professional footballers
- Fight, flight or finished: forced fitness behaviours in Game of Thrones
- Cardiorespiratory fitness predicts greater hippocampal volume and rate of episodic associative learning in older adults
- Does time spent in the residential neighbourhood moderate the relationship between neighbourhood walkability and transport-related walking? a cross-sectional study from Toronto, Canada
- Lifestyle and work ability in a general working population in Norway: a cross-sectional study
- 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
- 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
- A transcript-wide association study in physical activity intervention implicates molecular pathways in chronic disease
- Polygenic risk scores applied to a single cohort reveal pleiotropy among hundreds of human phenotypes
- Impact of first and second eye cataract surgery on physical activity: a prospective study
- Non-communicable disease risk factors: a call for primary care clinicians to act and to refer. Brief intervention, not silent abdication.
- Urban-rural differences in the association between blood lipids and characteristics of the built environment: a systematic review and meta-analysis
- Exercise Is Medicine: Primary Care Counseling on Aerobic Fitness and Muscle Strengthening
- Strength training as superior, dose-dependent and safe prevention of acute and overuse sports injuries: a systematic review, qualitative analysis and meta-analysis
- Distribution of diabetes, hypertension and non-communicable disease risk factors among adults in rural Bangladesh: a cross-sectional survey
- A Population-Based Study of the Bidirectional Association Between Obstructive Sleep Apnea and Type 2 Diabetes in Three Prospective U.S. Cohorts
- Exercise Training for Patients With Hypertrophic Cardiomyopathy: JACC Review Topic of the Week
- Assessment of cardiovascular risk and preparticipation screening protocols in masters athletes: the Masters Athlete Screening Study (MASS): a cross-sectional study
More in this TOC Section
Similar Articles