Abstract
Background: In Canada, more than 2 million people live with osteoporosis, a disease that increases the risk for fractures, which result in excess mortality and morbidity, decreased quality of life and loss of autonomy. This guideline update is intended to assist Canadian health care professionals in the delivery of care to optimize skeletal health and prevent fractures in postmenopausal females and in males aged 50 years and older.
Methods: This guideline is an update of the 2010 Osteoporosis Canada clinical practice guideline on the diagnosis and management of osteoporosis in Canada. We followed the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework and quality assurance as per Appraisal of Guidelines for Research and Evaluation (AGREE II) quality and reporting standards. Primary care physicians and patient partners were represented at all levels of the guideline committees and groups, and participated throughout the entire process to ensure relevance to target users. The process for managing competing interests was developed before and continued throughout the guideline development, informed by the Guideline International Network principles. We considered benefits and harms, patient values and preferences, resources, equity, acceptability and feasibility when developing recommendations; the strength of each recommendation was assigned according to the GRADE framework.
Recommendations The 25 recommendations and 10 good practice statements are grouped under the sections of exercise, nutrition, fracture risk assessment and treatment initiation, pharmacologic interventions, duration and sequence of therapy, and monitoring. The management of osteoporosis should be guided by the patient’s risk of fracture, based on clinical assessment and using a validated fracture risk assessment tool. Exercise, nutrition and pharmacotherapy are key elements of the management strategy for fracture prevention and should be individualized.
Interpretation: The aim of this guideline is to empower health care professionals and patients to have meaningful discussions on the importance of skeletal health and fracture risk throughout older adulthood. Identification and appropriate management of skeletal fragility can reduce fractures, and preserve mobility, autonomy and quality of life.
Fracture risk increases with advancing age, as a result of declining skeletal strength and increased risk of falling. In Canada, more than 2 million people live with osteoporosis.1 Every year in Canada, about 150 people per 100 000 suffer a hip fracture, which is considered among the most serious fractures associated with osteoporosis. Fractures lead to increased morbidity, excess mortality, decreased quality of life and loss of autonomy.2 Although osteoporosis is often considered a disease of older females, males are remarkably underevaluated and undertreated for the condition despite suffering worse outcomes following fracture,3 highlighting the importance of providing guidance in males.
Osteoporosis, defined as a bone mineral density (BMD) of 2.5 or more standard deviations below the peak bone mass (i.e., T-score ≤ −2.5), is an indicator of increased fracture risk; this risk is modified by age, sex and other factors.4 A clinical diagnosis of osteoporosis can be made in people aged 50 years and older if they have sustained a low-trauma hip, vertebral, humerus or pelvic fracture after the age of 40 years, or if they have an absolute fracture risk of 20% or more over the next 10 years, using a fracture risk assessment tool (FRAX or the Canadian Association of Radiologists and Osteoporosis Canada [CAROC]).5–7
Advances in risk assessment and nonpharmacologic and pharmacologic management warranted an update to the Osteoporosis Canada 2010 clinical practice guideline for the diagnosis and management of osteoporosis in Canada.8
Scope
Developed by the Osteoporosis Canada 2023 Guideline Update Group, this updated guideline is intended to assist Canadian primary health care professionals in screening community-dwelling postmenopausal females and males aged 50 years and older for the presence of risk factors for osteoporosis and fractures, and in providing interventions to optimize skeletal health and fracture prevention. Throughout the guideline, we use “females” and “males” to refer to biological sex.
The focus of the guideline recommendations for treatment is on people with primary osteoporosis. The guideline does not address the complexity of patients with cancer, serious illnesses or active conditions that can induce bone loss (e.g., hyperparathyroidism, multiple myeloma, or newly diagnosed rheumatoid arthritis or other inflammatory conditions requiring high-dose glucocorticoid therapy). Conditions known to cause secondary osteoporosis should be sought and referral to specialists with appropriate expertise for co-management considered (Appendix 1, Supplementary Table 5, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.221647/tab-related-content).
Falls are a leading cause of fractures among older adults in Canada.9 Because detailed recommendations for fall prevention were beyond the scope of this guideline, we refer the reader to guidance from the Canadian Task Force on Preventive Health Care on falls prevention.10 Specific recommendations on preventing fracture in people who reside in long-term care have been published.11
Recommendations
We formulated 25 recommendations and 10 good practice statements (GPS) using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework (Table 1). The recommendations are grouped under the sections of exercise, nutrition, fracture risk assessment and treatment initiation, pharmacologic interventions, duration and sequence of therapy, and monitoring.12,13
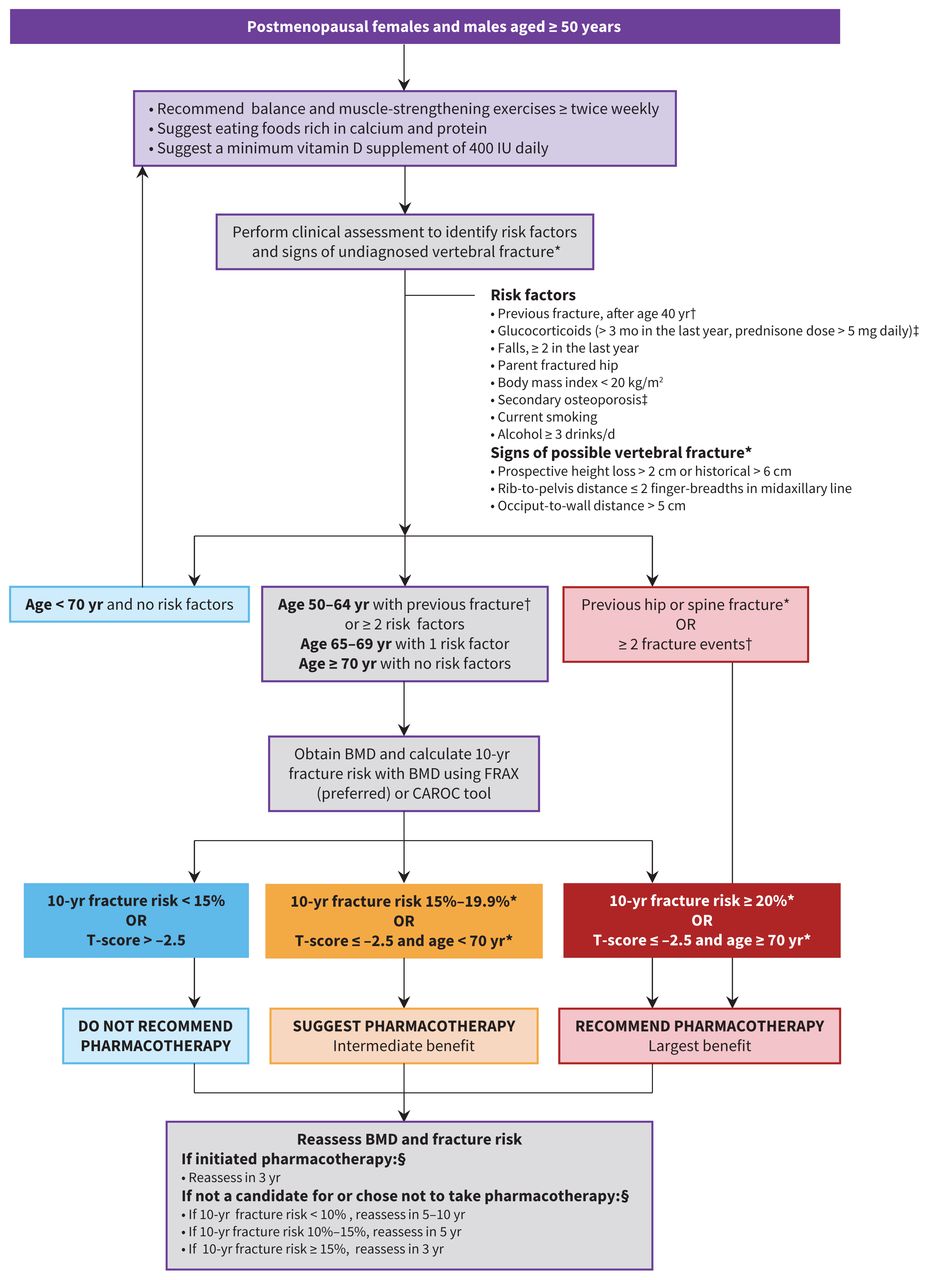
Figure 1 describes an integrated approach to bone health and fracture prevention in postmenopausal females and in males aged 50 years and older, and Figure 2 presents an approach to pharmacologic treatment, when required. Appendix 2 (available at www.cmaj.ca/lookup/doi/10.1503/cmaj.221647/tab-related-content) provides evidence-to-decision tables (starting on p. 50) that explain our rationales for strength of recommendations and certainty of evidence.
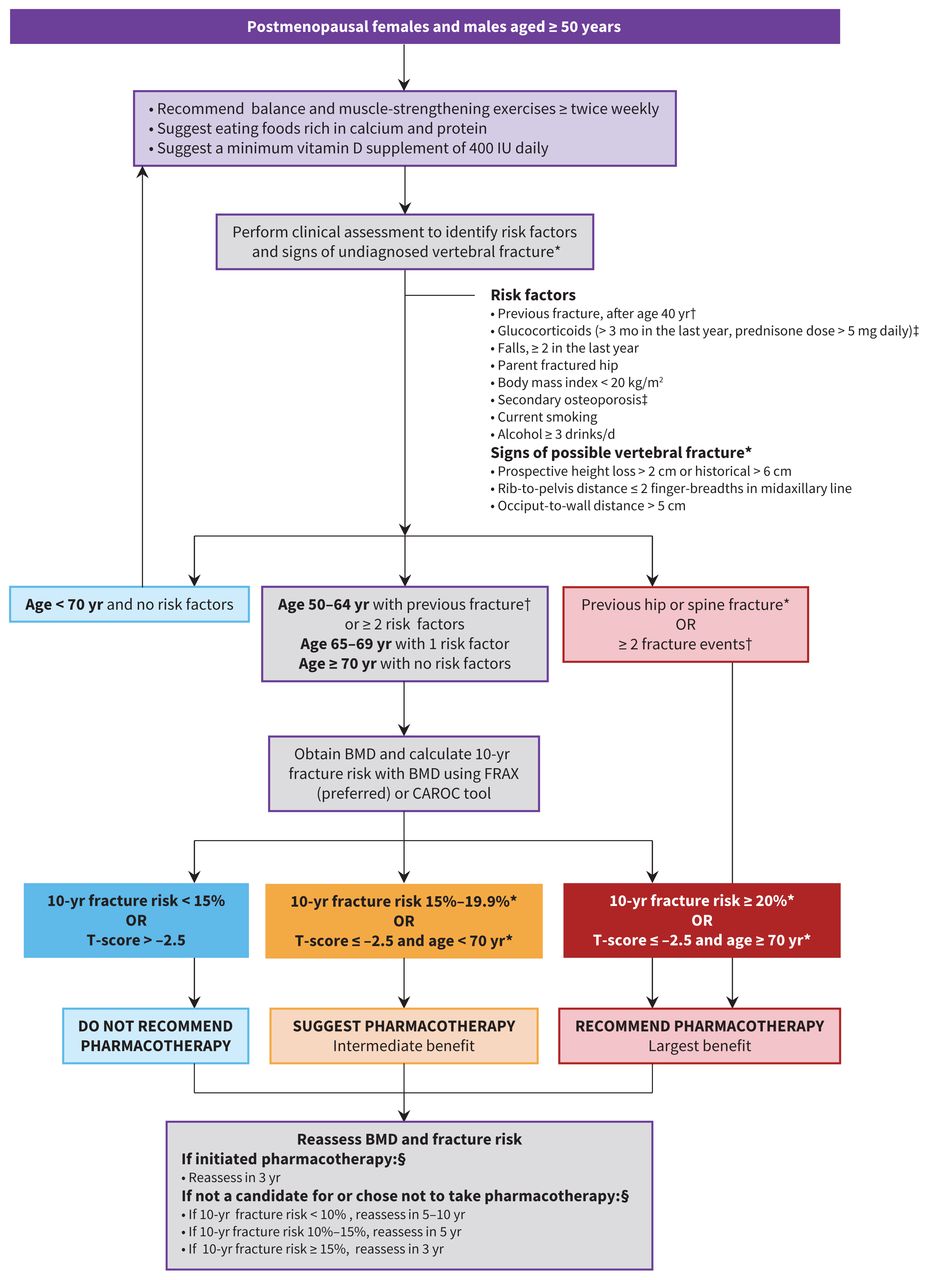
Integrated approach to the management of bone health and fracture prevention in postmenopausal females and males aged 50 years and older. See Appendix 1, Supplementary Tables 1–6 (available at www.cmaj.ca/lookup/doi/10.1503/cmaj.221647/tab-related-content) for more information on exercise and nutrition, secondary causes of osteoporosis and vertebral fracture assessment. Note: BMD = bone mineral density. *Consider lateral spine imaging to identify vertebral fracture(s). Finding of undiagnosed vertebral fracture(s) can guide appropriate choice and duration of therapy (Appendix 1, Supplementary Table 6). †Fractures that occur after the age of 40 years, in the setting of low trauma. Fractures of the hands, feet and craniofacial bones are not considered osteoporotic fractures. ‡Conditions known to cause secondary osteoporosis (Appendix 1, Supplementary able 5); consider referral to specialists with expertise for co-management. §Should be reassessed earlier if patient develops secondary causes (Appendix 1, Supplementary Table 5), new fracture or other risk factor for rapid bone loss.
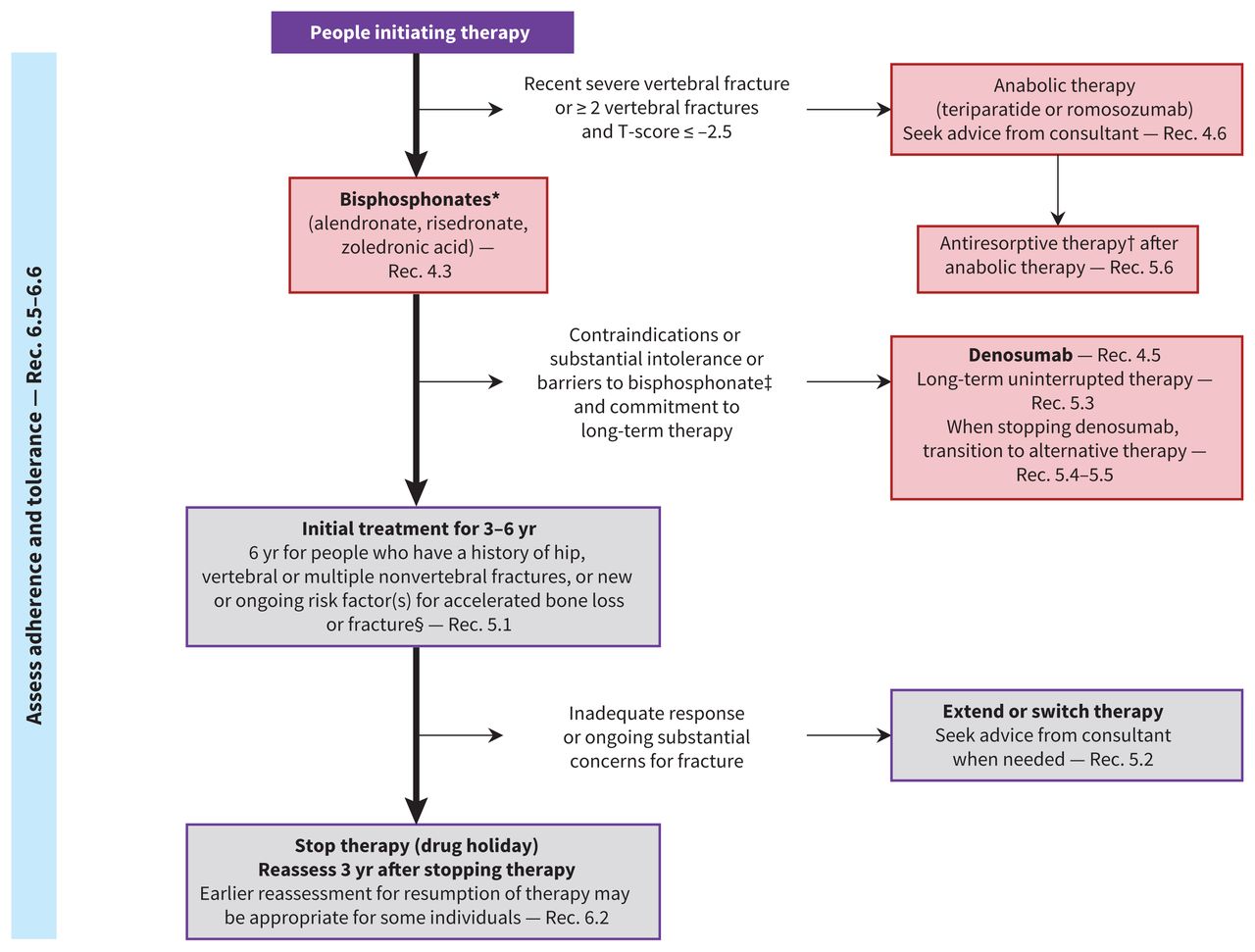
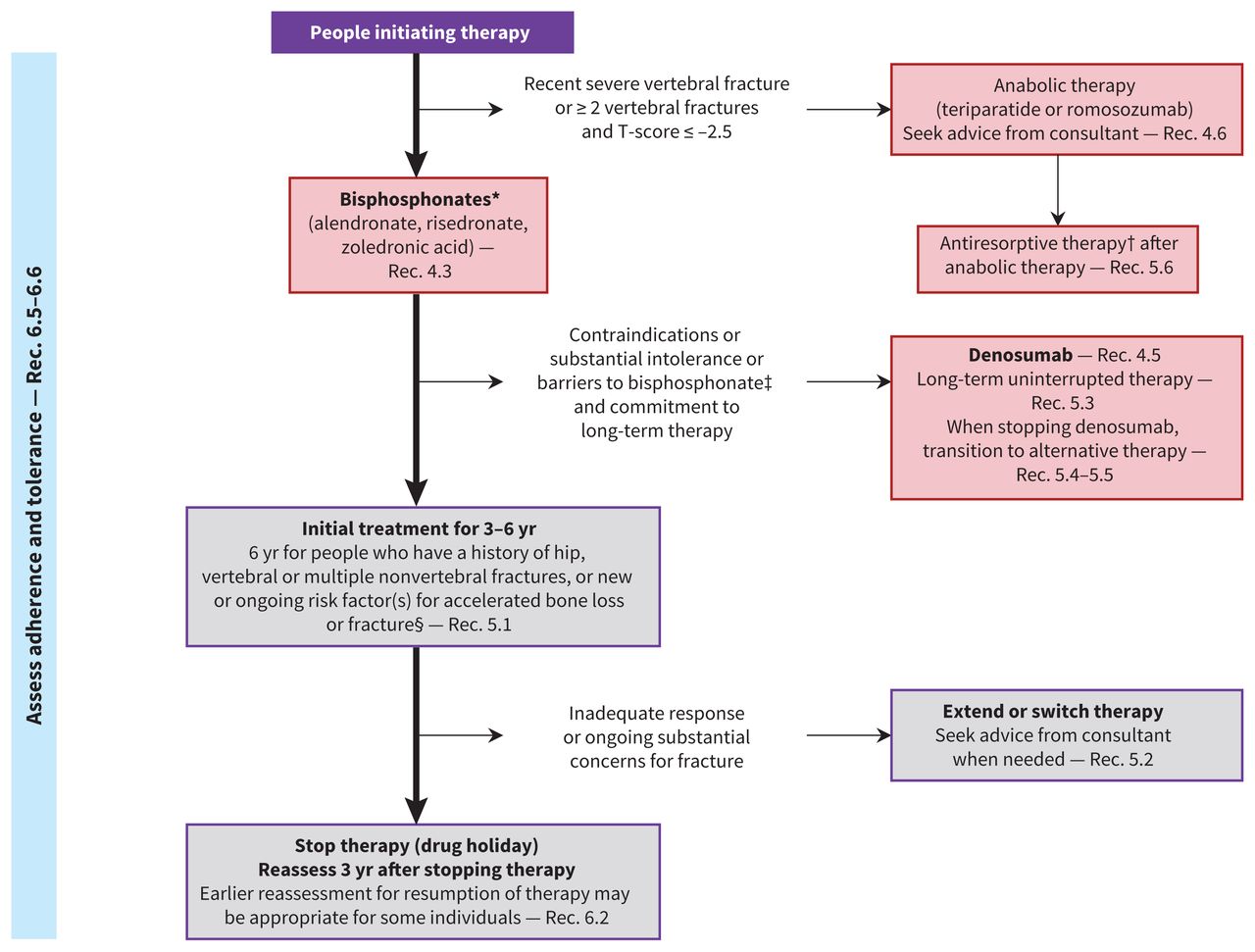
Approach to pharmacotherapy to prevent fractures. Note: Rec. = recommendation (see Tables 4, 6 and 7 for full recommendations). * Menopausal hormone therapy is a suggested alternative for females younger than 60 years or within 10 years after menopause who prioritize alleviation of substantial menopausal symptoms (Rec. 4.4). †Antiresorptive therapy includes bisphosphonates (alendronate, risedronate and zoledronic acid), denosumab, raloxifene and menopausal hormone therapy. ‡Raloxifene is suggested rather than no treatment for females who have contraindications or substantial intolerance to, or who choose not to take, other suggested therapies) (Rec. 4.7). §See Figure 1 for list of risk factors and Appendix 1, Supplementary Table 5, for causes of secondary osteoporosis.
We considered certainty of evidence, benefits and harms of interventions on clinical outcomes in the decision-making process. Males were under-represented in the clinical evidence of certain interventions and outcomes; we therefore report the strength of the recommendations based on the certainty of the evidence separately for males and females, where appropriate. All recommendations and GPS were informed by input from primary care physicians and patient partners, and include their values and preferences. Although for this guideline, we did not carry out cost-effectiveness analyses, we have considered cost-effectiveness information, when available, in the development of the recommendations and documented this in the specific evidence-to-decision tables.14–16
In adults older than 40 years, osteoporosis can result in fractures. Often referred to as fragility or osteoporosis-related fractures, they occur as a result of a fall from standing height or when the force applied to the bone is judged to be insufficient to fracture normal bone.17 Fractures of the hip, vertebra, humerus and distal forearm are categorized as major osteoporotic fractures, whereas fractures of the hands, feet and craniofacial bones are not considered osteoporotic fractures.1 Vertebral fractures, whether clinically silent or symptomatic, are associated with increased risk of fractures at all skeletal sites and can be identified or verified by radiologic imaging.18,19
Exercise
The recommendations on exercise for fall and fracture prevention for postmenopausal females and males aged 50 years and older are outlined in Table 2 (also see Appendix 1, Supplementary Table 1: key points on exercise and definitions). Evidence-to-decision tables are in Appendix 2 (p. 50).
Recommendations on exercise and nutrition for fall and fracture prevention in postmenopausal females and males aged 50 years and older*
High-quality evidence from a Cochrane systematic review shows that functional and balance training in adults older than 50 years can reduce the number of falls (rate ratio 0.76, 95% confidence interval [CI] 0.70–0.80; 41 studies, 7290 participants; high-certainty evidence) and the number of people who fall (rate ratio 0.87, 95% CI 0.82–0.91; 38 studies, 8288 participants; high-certainty evidence). Some evidence exists that functional and balance training may reduce the number of people who have fall-related fractures (rate ratio 0.44, 95% CI 0.25–0.76; 7 studies, 2139 participants; low-certainty evidence), and may improve quality of life (mean difference 2.48 points, 95% CI 1.31–3.64; 8 studies, 854 participants; low-certainty evidence) and physical functioning.20
A systematic review of randomized controlled trials (RCTs) suggests that resistance training may improve quality of life (standardized mean difference 0.75, 95% CI 0.54–0.95; 8 studies, 421 participants; moderate-certainty evidence), physical functioning and BMD, and reduce mortality.21 When combined with functional and balance training in older adults, resistance training can reduce the number of falls and number of people who fall.
Evidence from a systematic review of RCTs shows that in people with hyperkyphosis, exercises targeting abdominal, back extensor and shoulder muscles may result in small improvements in spinal curvature, quality of life, physical functioning and back extensor strength;22 however, effects on spinal curvature may not occur with fixed kyphosis (e.g., from vertebral fracture).
Observational studies suggest that walking may reduce mortality in older adults,23 but effects on fractures, falls, quality of life, physical functioning or harms in people at risk of fracture are unknown, or effects are uncertain.24 A systematic review suggests that impact exercise may improve BMD and physical functioning, and may reduce mortality,25 but the benefit of this type of exercise in isolation is uncertain, as it is often combined with resistance exercise or other exercise.
We performed systematic reviews on the effects of yoga and Pilates on health-related outcomes and found that these types of exercise may improve physical functioning and quality of life in older adults, but effects on BMD, falls and fractures are uncertain, and evidence for people at risk of fracture is limited.
Males were underrepresented in the evidence for some of the exercise outcomes. We chose not to downgrade the strength of the evidence for indirectness when applied to males because there was no reason to expect that the direction or magnitude of the effects on falls, fractures, physical functioning, quality of life or adverse events would be different in males.
Nutrition
Table 2 summarizes the recommendations on nutrition for postmenopausal females and males aged 50 years and older to prevent falls and fracture (Appendix 1, Supplementary Table 2: key points on nutrition). Evidence-to-decision tables are in Appendix 2 (p. 114).
For people who are consuming a balanced diet (https://food-guide.canada.ca/en/food-guide-snapshot/) and not receiving pharmacotherapy for osteoporosis, supplementation with calcium, vitamin D and protein is likely to have little to no beneficial or detrimental effect on fractures (Appendix 1, Supplementary Table 2). In systematic reviews and recent individual studies on calcium and vitamin D use, conducted predominantly in people not receiving osteoporosis pharmacotherapy and without deficiency, supplementation was associated with small, unimportant benefits in fracture reduction regardless of fracture site.26,27 Minimal decreases in falls were observed for vitamin D supplementation alone or in combination with calcium.27,28 Evidence for supplementation with magnesium and vitamin K in relation to bone health is limited (Appendix 2, p. 161).
Reduction in hip fracture rates with protein supplementation may be minimal.29,30 The evidence is uncertain because the studies assessed dietary rather than supplemental levels, often at or above the recommended level (0.8–1.3 g protein/kg body weight/d) and in people who were well nourished. Whether protein source matters with respect to bone health is unclear, because most participants had low intakes of plant protein. The effect on functional outcomes with higher dietary protein intakes was minimal.31
Fracture risk assessment
The recommendations on fracture risk assessment are presented in Table 3, with evidence-to-decision tables in Appendix 2 (p. 182). Figure 1 shows the clinical application of these recommendations.
Fracture risk assessment and treatment initiation in postmenopausal females and males aged 50 years and older*
We suggest an approach based on the assessment of age and the presence of clinical risk factors (i.e., a “targeted” approach) for identifying people who should undergo BMD measurement (low-certainty evidence in postmenopausal females aged 50–64 years; moderate-certainty evidence in females aged ≥ 65 years;32–34 very low-certainty evidence in males).14,32,35 This strategy delays BMD testing in most people until age 70 years and allows for appropriate categorization of those at high fracture risk with the fracture risk assessment tools available in Canada.32 Patient partners stated that providing guidance in identifying both females and males for appropriate BMD testing based on the presence of clinical risk factors was of high importance.
In Canada, validated 10-year major osteoporotic fracture assessment tools include FRAX and CAROC. FRAX’s performance is as good as or slightly better than that of other tools,36 and results in better fracture risk classification than CAROC (net reclassification improvement in risk category by 2% and in treatment recommendation by 1%).37 We suggest the use of the Canada-specific FRAX tool as the preferred tool for fracture risk estimation; however, this recommendation is conditional, owing to the moderate certainty of the evidence and indirectness of evidence in males.37
Treatment initiation
Recommendations on initiating treatment are provided in Table 3, with evidence-to-decision tables in Appendix 2 (p. 190 and p. 314).
No consensus exists on the optimal approach to setting a treatment threshold.38 In setting pharmacotherapy initiation thresholds, we considered the burden of fractures in the Canadian population, how fracture outcomes were affected by baseline fracture risk, the efficacy of pharmacotherapy on fracture outcomes, the importance of identifying those at high fracture risk to prevent the most fractures and the importance of limiting overtreatment in those at lower risk, from population and patient perspectives.38
Previous fracture of the vertebra (clinical or documented on imaging) or the hip, and more than 1 fracture, indicate high risk for future fractures.8 Randomized controlled trials provide a moderate-to-high certainty of evidence showing important benefits of fracture reduction with pharmacotherapy in people with osteoporosis (defined as T-score ≤ −2.5 or history of previous fracture), with a risk reduction of about 50% for vertebral, 30% for hip, and 20% for nonvertebral fractures after 3 years of treatment.39–41 In addition, given observational data from a large clinical registry, an intervention threshold of 20% for 10-year major fracture risk (as measured by FRAX or CAROC) was also selected (as a conditional recommendation), as this strategy was highly ranked in terms of number of fractures prevented among females aged 50 years and older and the number of females treated (to limit overtreatment).38 We did not rate down the certainty of the evidence in males, as evidence suggests that there are no differences in treatment benefits and harms by sex.39,41–44
Fracture Liaison Service programs (https://fls.osteoporosis.ca/), which provide postfracture investigation and treatment initiation and are currently in place in a few Canadian jurisdictions, increase the appropriate use of fracture risk assessment and antifracture treatment, and are cost-effective.45 We recommend that postmenopausal females and males aged 50 years and older who present with a recent fracture have access to a Fracture Liaison Service to improve identification and treatment initiation for osteoporosis.
Pharmacologic interventions
Table 4 presents the recommendations on pharmacotherapy in those initiating therapy (additional information in Table 5), with an algorithm for clinical application in Figure 2. Evidence-to-decision tables are in Appendix 2 (p. 323).
Pharmacologic interventions for postmenopausal females and males aged 50 years and older for whom anti-osteoporosis treatment is recommended or suggested*
Medications for the treatment of osteoporosis*
Pharmacologic therapies are classified as antiresorptive therapy, which inhibits osteoclastic activity, and anabolic therapy, which stimulates new bone formation. Antiresorptive therapy includes bisphosphonates (alendronate, risedronate and zoledronic acid), denosumab, raloxifene and menopausal hormone therapy; anabolic therapy includes teriparatide and romosozumab (Table 5).
There was evidence of moderate-to high certainty in pharmacotherapy effects.39 Although most studies were performed in postmenopausal females, the evidence available in males with primary or hypogonadal osteoporosis shows similar effects to females on fractures with bisphosphonates and denosumab; therefore, the evidence from females was used for males but rated as moderate certainty from some indirectness.39,41,42
Overall, bisphosphonate therapy for 3 years results in 20–30 fewer vertebral, 10 fewer nonvertebral, and 3 fewer hip fractures per 1000 people than no treatment.39,41 Compared with placebo, there may be very few harms with short-term (≤ 3 yr) use of oral bisphosphonate therapy, including gastrointestinal events such as esophagitis and ulcers (< 1% difference), and transient flu-like symptoms with zoledronic acid infusions, as well as very uncertain evidence for an increased risk of atrial fibrillation.43 The benefits of denosumab are similar to those of zoledronic acid,39 but there may be greater harms with denosumab: 7% more serious adverse events (such as infections requiring hospital admission) than with placebo47 and 14% and 7% more when compared with alendronate and zoledronic acid, respectively. 15 Delayed dosing or discontinuation of denosumab is associated with rapid bone loss and may lead to vertebral fractures.52
In females with higher risk of fractures (e.g., recent severe vertebral fracture, or > 1 vertebral fracture and T-score ≤ −2.5),53 there is high-certainty evidence that anabolic therapy (teriparatide or romosozumab) results in greater reductions in vertebral, nonvertebral and hip fractures than bisphosphonates (35, 18 and 5 fewer, respectively, per 1000 people).39,43 This evidence is indirect in males and therefore of moderate certainty. Stopping anabolic treatment without subsequent antiresorptive therapy risks the loss of bone density gains.54,55 For most people, the downsides of teriparatide, romosozumab or denosumab (such as injection schedules, the risks associated with and need for transition therapy when stopping the medication, and costs) probably outweigh the benefits compared with bisphosphonates.56 However, for people at higher risk of fractures, the benefits may outweigh these downsides.
Duration and sequence of therapy
Recommendations on duration and sequence of therapy are outlined in Table 6. Evidence-to-decision tables are in Appendix 2 (p. 330).
Duration and sequence of therapy in postmenopausal females and males aged 50 years and older who receive anti-osteoporosis medications*
Taking oral bisphosphonates for 5 years or more (e.g., for as long as 10 yr in the oral alendronate extension study57), compared with shorter durations, likely results in no difference in hip or overall number of fractures, but a moderate-to-small reduction in clinically (22 fewer per 1000) and radiologically (17 fewer per 1000) identified vertebral fractures.43,58 Taking zoledronic acid annually for 6 years, compared with 3 years annually, likely results in no difference in hip and nonvertebral fractures, but radiologically confirmed vertebral fractures may be substantially reduced, although the evidence is uncertain (56 fewer per 1000, from 88 to 5 fewer).48
Harms may be increased with longer durations of bisphosphonates: after 6 years, there are 39–131 atypical femur fractures (a stress or insufficiency fracture occurring in the femoral shaft) per 100 000 person-years, compared with 25 at 3–5 years, and higher risk in females who self-report Asian race or ethnicity;49 and the risk of osteonecrosis of the jaw (a condition in which ≥ 1 parts of the jaw bone becomes necrotic and exposed to the oral cavity) is 25 per 100 000 person-years, and approximately doubles with use longer than 5 years.50 At 6 years, these harms likely outweigh the benefits of continued therapy, except in people at higher risk of fractures (e.g., previous hip or vertebral fractures, recent fracture, multiple fractures).
Evidence suggests that the benefits of denosumab do not wane at 10 years of therapy and the incidence of atypical femur fracture and osteonecrosis of the jaw is relatively stable at 8 and 52 per 100 000 patient-years, respectively.51 There are insufficient data comparing the effects of continuing or switching medications when there is concern of inadequate response to bisphosphonates (e.g., substantial BMD decline).59–62
Monitoring
Table 7 presents the recommendations on monitoring in patients who initiate pharmacotherapies or stop bisphosphonates. Evidence-to-decision tables are in Appendix 2 (p. 249).
Monitoring of therapy in postmenopausal females and males aged 50 years and older who receive anti-osteoporosis medication*
Very low-certainty direct and strong indirect evidence in females and males support a possible improvement in fracture risk in people who undergo BMD monitoring about 3 years after initiation of therapy.63,64 Bone turnover markers measure the remodelling process (e.g., C-terminal telopeptide of type 1 collagen for bone resorption and bone-specific bone alkaline phosphatase for bone formation).65 Inadequate evidence exists to support the clinical use of bone turnover markers to reduce fracture risk or to predict fracture in those on a bisphosphonate drug holiday.66
Methods
This guideline was developed by the volunteer Osteoporosis Canada 2023 Guideline Update Group to address advances in risk assessment, nonpharmacologic and pharmacologic osteoporosis management since the publication of the 2010 Osteoporosis Canada guideline.8 We followed the GRADE framework13 and quality assurance as per Appraisal of Guidelines for Research and Evaluation (AGREE II) quality and reporting standards.67 We began the guideline work in June 2017 and completed it in November 2022.
Guideline panel composition
The Osteoporosis Canada 2023 Guideline Update Group consisted of a steering committee (S.N.M., S.K., N.S., S.F., L.G., W.W., H.M.-B. [ex officio] and L.F.) selected by the Osteoporosis Canada Scientific Advisory Council, a conflict-of-interest oversight committee (H.M.-B., L.F. and R.R.), 4 working groups (chairs: exercise [L.G.], nutrition [W.W.], fracture risk assessment [S.F.], pharmacotherapy [S.K. and N.S.]) and a knowledge translation committee. Primary care physicians and 5 patient partners were represented on the steering committee and were on the working groups, to ensure relevance to target users. A methodologist (N.S.) with expertise in guideline development and GRADE methodology was a member of the steering committee and the Pharmacotherapy Working Group, and consulted with the other working groups.
The steering committee was responsible for the organization of the guideline processes, setting of priorities, recruiting of working group participants, oversight of the working group activities and preparation for publication. We applied the principles of equity, diversity and inclusion in the recruitment of working group participants, ensuring appropriate representation for the following: sex, age, expertise (e.g., physicians, pharmacists, physiotherapists, nutritionist, patient partners) and location in Canada. Working group chairs were tasked with recruiting participants to their group with support from the steering committee. We recruited patient partners from the Canadian Osteoporosis Patient Network across the country (https://osteoporosis.ca/copn-patient-network/).
Selection of priority topics
We established the priority areas and all research questions from surveys of more than 1000 patient partners68 and primary care physicians, and through direct input from people with lived osteoporosis experience, primary care physicians and bone health experts at an initial face-to-face meeting (June 2, 2017; 35 attendees). Each working group formulated questions using the PICO framework (patient, intervention, comparison, outcome), which the steering committee then reviewed (Appendix 2, Questions, p. 22).
Outcomes of interest comprised hip fractures, vertebral fractures, all fractures, fracture-related mortality, physical functioning and disability, quality of life or well-being, and harms such as adverse events from medication, including atypical femur fractures and osteonecrosis of the jaw.68 The Exercise Working Group also considered falls. We agreed, through consensus, on the variation in absolute risk that would be considered clinically important by patients and clinicians, depending on the outcome (Appendix 2, Outcomes of Interest, p. 20).
Literature search and quality assessment
We conducted literature searches (Appendix 2, Search Strategies, p. 27), initially looking for recent systematic reviews of RCTs. In the absence of recent systematic reviews, we conducted a systematic review of the primary literature (initially of RCTs and, if not available, of observational studies).21,22,24,25,69,70 Each working group had the support of a research librarian for the search strategies. The development of certain recommendations was supported by the results of analyses from a large observational Canadian cohort registry (the Manitoba Bone Mineral Density registry).32,38 We searched for systematic reviews for patient values and preferences. We considered indirect evidence when direct evidence was not available or was of very low quality.
The latest systematic search dates were October 2020; each working group surveyed the literature for pertinent RCTs until the fall of 2022 (or publication of their systematic reviews, as for the Exercise Working Group). We verified the results of the searches for the presence of retracted articles (Appendix 2, Pharmacotherapy Working Group, p. 49). Each working group summarized the evidence, appraised it for biases and developed evidence-to-decision tables (Appendix 2, Evidence-to-Decision Tables, p. 50).
Development of recommendations
After the development of the evidence-to-decision tables, each working group formulated the recommendations using the GRADE framework.13 The working groups considered benefits and harms, patient values and preferences, resources, equity, acceptability and feasibility when making decisions and presented their initial work at a face-to-face meeting (Nov. 15, 2019; 28 attendees). Initial decision-making on the recommendations took place separately in each working group, by voting (email or using GRADEpro software [https://gradepro.org]) or by consensus, depending on the working group size and its membership.
The strength of each recommendation was assigned according to the GRADE system, as strong (“We recommend …”) or conditional (“We suggest …”) (Table 1). Some recommendations met the GRADE Working Group criteria for GPS, where the guideline group agreed that the benefits of implementing the GPS would result in large positive consequences (even if supported by indirect evidence), and did not require further collection and summary of the evidence.12 Recommendations and GPS from each working group were reviewed and approved by the steering committee and thereafter by the Osteoporosis Canada 2023 Guideline Update Group as a whole.
External review
Relevant stakeholders (Appendix 2, Stakeholder Participants, p. 18), as determined by the steering committee, provided feedback in October 2022 regarding clarity and clinical utility of the recommendations. Each working group collated and reviewed feedback received for the recommendations they had developed; the steering committee then reviewed the suggested changes and incorporated them as appropriate into the guideline, followed by review and approval from the Osteoporosis Canada 2023 Guideline Update Group.
Management of competing interests
The process for managing competing interests was developed before and continued throughout the guideline development, informed by Guideline International Network principles and overseen by the conflict-of-interest oversight committee (Appendix 2, Conflict of Interest, p. 6).71 Working group chairs and at least half of each working group’s membership were required to be free of financial competing interests during the guideline development process. Members with financial competing interests were excluded from formulating and voting on recommendations. Competing interests were adjudicated via annual submission by email (Appendix 2, Annual Conflict-of-Interest Declaration Template, p. 12) to the conflict-of-interest oversight committee and by verbal updates to respective chairs at each working group meeting.
Funding came from the Canadian Institutes of Health Research (Planning and Dissemination Grant program 2017) and Osteoporosis Canada. Osteoporosis Canada, a patient-focused organization, supports, educates and advocates at the individual, community and governmental levels regarding bone health, fracture risk reduction and management strategies for osteoporosis. It receives about 8% of its funding from corporations and foundations (including pharmaceutical industry and lobby groups) and the remainder from government sources (68.5%), individuals (23%) and other (0.5%) (https://osteoporosis.ca/our-impact/).
We managed the funders’ competing interests through an arm’s-length relationship with Osteoporosis Canada leadership or staff, who did not sit on committees nor any of the working groups. The funding sources had no direct contact with any member of the steering committee or working groups. The views of the funding bodies did not influence the process, nor the content of the recommendations of the guideline. Funding supported research librarians via Cochrane Canada and the GRADE methodologist at McMaster University via institutional mechanisms.
Implementation
We are developing knowledge transfer tools to support patients and clinicians in their discussions on exercise, nutrition, fracture risk and osteoporosis treatment, including a free digital mobile application to provide point of care and educational support (https://osteoporosis.ca/). We will ensure timely dissemination of the tools and guideline content through the Osteoporosis Canada website and network, podcast, and initiatives with patients and primary care providers. Osteoporosis Canada will monitor downloads of the digital application, traffic to its website, the Canadian FRAX tool and implementation of the guideline recommendations in Fracture Liaison Services across the country.
Updates will be published as peer-reviewed, structured guidance statements when new data pertinent to clinical assessment and management of osteoporosis emerge.
Other guidelines
Changes from the 2010 Osteoporosis Canada guideline8 include the use of the GRADE framework in the development of the recommendations, the addition of expanded recommendations on exercise and types of exercise, and guidance on nutrients other than calcium and vitamin D. We also provide clearer guidance on thresholds for treatment initiation, duration of therapy and monitoring.
Based on evidence from a systematic review of RCTs, the Canadian Task Force on Preventive Health Care guideline recommends risk assessment — first screening for the primary prevention of fragility fractures in females aged 65 years and older with the initial application of the FRAX tool without BMD.72 The task force guideline recommends against screening younger females and males of any age. Of note, the task force’s recommendations apply to community-dwelling people who are not on anti-osteoporosis pharmacotherapy.
The United States Preventive Services Task Force found convincing evidence for the accuracy of BMD measurements and risk assessment tools at identifying risk of osteoporotic fractures, and that drug therapies reduce fracture rates in postmenopausal females.73 The US Bone Health and Osteoporosis Foundation uses a similar approach as our update, to screening (i.e., screening postmenopausal females and males aged ≥ 50 yr with a history of fracture or clinical risk factors) and recommends treatment based on any of the following: vertebral or hip fracture; humerus, pelvis or distal forearm fracture with low bone mass; a BMD T-score ≤ −2.5; and low bone mass and a US FRAX 10-year probability of a hip fracture ≥ 3% or of major osteoporosis-related fracture ≥ 20%.74 The United Kingdom National Osteoporosis Guidelines Group uses a 2-step screening process for identifying people at high fracture risk, with age-dependent cut-offs for pharmacologic intervention.75 Most clinical guidelines recommend vertebral fracture assessment in people with selected risk factors.74,76
Recent guidelines, such as those of the American College of Physicians, the US Bone Health and Osteoporosis Foundation, and the UK National Osteoporosis Guidelines Group, recommend bisphosphonates as first-line therapy in postmenopausal females and males with osteoporosis, whereas denosumab and anabolic therapies are mostly suggested as second-line therapy for people with intolerance, contraindications or higher risk.44,74,75,77 In addition, these guidelines support adequate calcium and vitamin D intake, and exercise for falls and fracture reduction.
Gaps in knowledge
More evidence is required to guide management in males and with regard to optimal screening of younger people (age 50–64 yr) for fracture risk reduction. The FRAX and CAROC tools have not been validated in transgender and gender-nonconforming people. Dietary patterns and the optimal level of dietary protein for fracture prevention are areas for future study. Further research is also warranted on duration of pharmacotherapy, bisphosphonate interruptions, and sequence of treatments, particularly in those who remain at high risk for fracture.
Limitations
We were not able to incorporate all topics of high relevance to skeletal health, such as fall prevention or identification of frailty, within this guideline. We also recognize that primary health care professionals may care for people with secondary causes of osteoporosis and multiple comorbidities. However, we determined that these situations were beyond the scope of this guideline, as they would require additional expertise, and therefore we recommended consultation with a specialist as feasible.
Although we did not update our searches of the literature on an ongoing basis (such as in living guidelines), we did keep abreast of any new or pivotal trials before publication. For some recommendations, we used indirect evidence to inform our guidance (e.g., screening, treatment and monitoring in males). In addition, we made recommendations based on magnitude of effects on fractures and harms that we assessed to be clinically important a priori, through consensus. We consider our guideline group was representative and would reflect values important to people at risk of fractures.
Conclusion
The aim of this guideline is to empower health care professionals and patients to have meaningful discussions on the importance of skeletal health and fracture risk in older adulthood. Identification and appropriate management of skeletal fragility in Canadians can reduce fractures, and preserve mobility, autonomy and quality of life in this population.
Acknowledgements
The authors thank the support team for their dedication to the guideline project and acknowledge their contributions. Fracture risk assessment working group: Hajar Abu Alrob, Arnav Agarwal, Lindsie Blencowe, Marija Djekic-Ivankovic and Jeevitha Srighanthan. Exercise working group: Zachary Fielding, Seyedeh Zeinab Hosseini, Kawon Victoria Kim and Emily McLaughlin. Nutrition working group: Ina Ilse. Pharmacotherapy working group: Lindsay Wong. Project administrative liaison: Kerry Grady (Osteoporosis Canada). Research librarians: Yuhong Yuan (McMaster University) and Jackie Stapleton (University of Waterloo). The authors thank the external reviewers and stakeholders (named in Appendix 2, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.221647/tab-related-content) for their contributions to the guideline.
Footnotes
Competing interests: Lora Giangregorio reports receiving an honorarium from Amgen Inc. for a lecture on exercise with no mention of medications, outside the current manuscript. Dr. Giangregorio is also a member of the Scientific Advisory Council of Osteoporosis Canada and co-lead of the Vertebral Fracture Special Interest Group, Fragility Fracture Network. Sandra Kim reports receiving support from Osteoporosis Canada for a Grading of Recommendations, Assessment, Development and Evaluations (GRADE) methodologist at McMaster University, during the conduct of the study. Dr. Kim was also a volunteer member of the Osteoporosis Canada Board of Directors from 2017 to 2020. Nancy Santesso reports receiving payment to provide GRADE expertise for guideline development and preparation of materials paid to institution (McMaster University), during the conduct of the study. Dr. Santesso has also received support from Osteoporosis Canada for travel to guideline-related meetings. Heather McDonald-Blumer reports receiving consulting fees from Eli Lilly and Novartis, for attendance on advisory boards, outside the submitted work. Rowena Ridout has been a member of the Osteoporosis Canada Board of Directors since 2020 (no payment received). Neil Binkley reports receiving a research grant (paid to institution) from Radius, and consulting fees and honoraria from Amgen. Angela Cheung has received honoraria for consultancy work from Amgen and Paladin Laboratories. Dr. Cheung has also held the following roles: member of the Clinical Guidelines Committee of the Endocrine Society; co-chair of the postmenopausal health pathway, American College of Obstetrics and Gynecology; and vice-president and co-chair of the 2023 Position Development Conference, International Society for Clinical Densitometry. Robert Josse reports receiving consulting fees from Amgen Canada, Paladin Laboratories and Alexion, and honoraria from Amgen and Alexion. Dr. Josse has also participated on advisory boards for Amgen, Paladin, Alexion and Ultragenyx. Aliya Khan has received research grants from Alexion, Amgen Canada, Takeda, Ascendis, Chugai, Radius, Amolyt and Ultragenyx, and speaker honoraria from Amgen, Alexion, Ascendis, Takeda and Ultragenyx. Dr. Khan has also participated on advisory boards for Amgen Canada, Alexion, Amolyt, Ascendis and Takeda. E. Lynn Izumi Nash reports receivin an honorarium from the Ontario College of Family Physicians for designing continuing medical education workshops on osteoporosis. Dr. Nash is also a member of the Scientific Advisory Council for Osteoporosis Canada (voluntary unpaid position). Zahra Bardai reports receiving honoraria as a member of the Pri-Med Canada Scientific Planning Committee (2011–present) and as an author of the Foundation for Medical Practice Education Small Group Practice–Based Learning Program, at McMaster University. Dr. Bardai is also a volunteer member of the Osteoporosis Canada Scientific Advisory Council. Suzanne Cadarette reports receiving research funds (paid to institution) as co–principal investigator on Canadian Institutes of Health Research and National Institutes of Health project grants. Heather Frame is a former member of the Osteoporosis Canada Board of Directors (term ended November 2020). Kaleen Hayes reports receiving researcher-initiated grants from the National Institute on Aging, Insight Therapeutics, Genentech and Sanofi (all paid directly to institution), and consulting fees from the Canadian Agency for Drugs and Technologies in Health. Alexandra Papaioannou has participated on an advisory board and in speakers’ bureaus and received honoraria from Amgen Canada. Christine Thomas has been a member of the Osteoporosis Canada Board of Directors at various time points.
This article has been peer reviewed.
Steering Committee: Suzanne N. Morin (chair), Sidney Feldman, Larry Funnell, Lora Giangregorio, Wendy Ward, Sandra Kim, Nancy Santesso, Heather McDonald-Blumer (ex-officio).
Conflict-of-Interest Oversight Committee: Heather McDonald-Blumer (Chair), Larry Funnell, Rowena Ridout.
Stakeholder Committee: Heather McDonald-Blumer (chair), Rowena Ridout, Larry Funnell.
Fracture Risk Assessment Working Group: Sidney Feldman (chair), Neil Binkley, Steven Burrell, Angela M. Cheung, Carol Holmes, George Ioannidis, Robert Josse, Aliya A. Khan, Virginia McIntyre, Suzanne N. Morin, Lynn Nash, Ahmed Negm, Lianne Tile.
Exercise Working Group: Lora Giangregorio (chair), Maureen C. Ashe, Zahra Bardai, Joan Bartley, Debra Butt, Phil Chilibeck, Isabel B. Rodrigues, Lehana Thabane, Matteo Ponzano, John D. Wark.
Nutrition Working Group: Wendy Ward (chair), William Gittings, Lynn Nash.
Pharmacotherapy Working Group: Sandra Kim (co-chair), Nancy Santesso (co-chair), Suzanne M. Cadarette, Sheila Dunn, Jamie Falk, Heather Frame, Kaleen Hayes, Susan B. Jaglal, Alexandra Papaioannou, Rowena Ridout, Christine A. Thomas.
Contributors: All of the authors made substantial contributions to the conception and design of the work, as well as acquisition, analysis and interpretation of data. Members of the Steering Committee wrote the first draft and all of the authors contributed to subsequent versions of the manuscript, including reviewing them critically for important intellectual content. All of the authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Funding came from the Canadian Institutes of Health Research (Planning and Dissemination Grant program, 2017), and Osteoporosis Canada. The views of the funding bodies did not influence the process, the content of this guideline or the preparation of the manuscript.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
Article extras
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections