Abstract
Background: Cancer surveillance data are essential to help understand where gaps exist and progress is being made in cancer control. We sought to summarize the expected impact of cancer in Canada in 2024, with projections of new cancer cases and deaths from cancer by sex and province or territory for all ages combined.
Methods: We obtained data on new cancer cases (i.e., incidence, 1984–2019) and deaths from cancer (i.e., mortality, 1984–2020) from the Canadian Cancer Registry and Canadian Vital Statistics Death Database, respectively. We projected cancer incidence and mortality counts and rates to 2024 for 23 types of cancer, overall, by sex, and by province or territory. We calculated age-standardized rates using data from the 2011 Canadian standard population.
Results: In 2024, the number of new cancer cases and deaths from cancer are expected to reach 247 100 and 88 100, respectively. The age-standardized incidence rate (ASIR) and mortality rate (ASMR) are projected to decrease slightly from previous years for both males and females, with higher rates among males (ASIR 562.2 per 100 000 and ASMR 209.6 per 100 000 among males; ASIR 495.9 per 100 000 and ASMR 152.8 per 100 000 among females). The ASIRs and ASMRs of several common cancers are projected to continue to decrease (i.e., lung, colorectal, and prostate cancer), while those of several others are projected to increase (i.e., liver and intrahepatic bile duct cancer, kidney cancer, melanoma, and non-Hodgkin lymphoma).
Interpretation: Although the overall incidence of cancer and associated mortality are declining, new cases and deaths in Canada are expected to increase in 2024, largely because of the growing and aging population. Efforts in prevention, screening, and treatment have reduced the impact of some cancers, but these short-term projections highlight the potential effect of cancer on people and health care systems in Canada.
Cancer has a substantial impact on the lives of people living in Canada and on Canadian health care systems.1,2 Previous estimates suggest that 45% of all people in Canada will receive a cancer diagnosis in their lifetime.3,4 As the population grows and ages, new cancer cases and deaths from cancer in Canada are also increasing.5,6 In addition, cancer has a major economic impact. The most recent estimates indicated that the economic burden of cancer in Canada was $26.2 billion in 2021, with 30% of costs being carried by patients and their families.7
Because of the time required for collecting and verifying data, cancer data necessarily lag several years. Short-term projections are estimated by extrapolating past trends into the future using statistical models. These projections of incidence and mortality provide a timely picture of the impact of cancer in Canada that is necessary for resource planning, research, and informing cancer control programs. Given the overall impact of cancer on the lives and economic livelihood of people in Canada, such estimates are essential to highlight where progress has been made in cancer control and where more resources and effort are required.
The Canadian Cancer Statistics 2023 included detailed estimates of cancer metrics, including incidence, mortality, survival by sex assigned at birth, age, and province or territory, as well as time trends, for 23 cancer types, from 1984 to 2023.3 We sought to update these analyses and determine projections of the counts and age-standardized rates of new cancer cases and deaths expected in 2024, by sex and by province or territory for all ages combined.
Methods
Study design
We conducted an analysis of population-level cancer data with updated projected estimates from the Canadian Cancer Statistics Advisory Committee, a collaboration between Statistics Canada, the Public Health Agency of Canada, and the Canadian Cancer Society. The advisory committee includes representation from each of these organizations, as well as representatives from the Canadian Partnership Against Cancer, provincial cancer registries, and academic collaborators. Analytical and methodological decisions are made collaboratively and agreed upon by the committee based on documented approaches.3 Unless otherwise noted, the data sources and methodical decisions used in this study are as described in detail in Canadian Cancer Statistics 2023.3
Sources of data
We obtained data on cancer incidence from the National Cancer Incidence Reporting System (1984–1991) and the Canadian Cancer Registry Tabulation Master File (1992–2019), released May 16, 2023.8 We obtained data on deaths from the Canadian Vital Statistics Death Database (1984–2020), released Jan. 24, 2022.9 These national population-based databases are populated by data submissions from provincial and territorial cancer registries to Statistics Canada, where these databases are maintained. We also obtained actual and projected population estimates from Statistics Canada.10–12
Statistical analysis
We projected counts and rates from 2020 to 2024 using the CANPROJ projection package to generate estimates of cancer incidence and mortality.13 The CANPROJ package uses trends in actual (i.e., historical) data to select the best-fit model for subsequent years based on a decision algorithm that compares 6 models, including the Nordpred (age–period–cohort drift), age–cohort, hybrid age-specific trend, hybrid age-common trend, hybrid age-only, and 5-year average models. Model selection is based on statistical tests for each model, starting with the most complex (Nordpred). Based on specific rules, a simpler model may be selected. Additional details on the CANPROJ modelling approach and model selection are provided in Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.240095/tab-related-content. Validation of the CANPROJ software has been completed using data on cancer incidence in Canada (excluding Quebec).14
The Canadian Cancer Statistics Advisory Committee reviewed each model selected by the CANPROJ software, alongside the 5 other models produced, to suggest the most appropriate model for each jurisdiction. The committee is guided by a set of principles, along with use of a decision tree, in making its recommendation (Appendix 1). Decisions on the final models for each province or territory were made by consensus in consultation with that jurisdiction’s cancer registry. For these analyses, we used the same models selected for Canadian Cancer Statistics 2023.3
For Quebec, we calculated incidence projections from 2018 to 2024 as cancer cases diagnosed in this province after 2017 had yet to be submitted to the Canadian Cancer Registry. In addition, Quebec transitioned from a registry exclusively based on hospital discharge data to a more integrated central registry, resulting in an artifactual increase for some type-specific cancer counts during the early years of the transition (2011–2012). Consequently, for these 2 diagnosis years, for some age- and sex-specific rates in Quebec, we used estimates derived from locally estimated scatterplot smoothing to the 2006–2017 reference period (Appendix 1). We generated incidence projections for Nova Scotia from 2019 to 2024, because the data for 2019 (i.e., submission of cases from the province to the Canadian Cancer Registry) required further verification.
We generated projected estimates for 23 cancer types by sex assigned at birth (hereafter referred to as sex) and geographic region (province or territory). Definitions of cancer types are in Appendix 1, Supplementary Table 1.15–17 We computed projected estimates for Canada as sums of the projections for each individual province and territory. All incidence and mortality rates were age-standardized to the 2011 Canadian standard population using the direct method.18
Ethics approval
Because this study involved the analysis of administrative data publicly available in Statistics Canada’s Research Data Centres and did not involve contacting individuals, consideration and approval by an ethics review board were not required.
Results
Incidence in 2024
In 2024, 247 100 new cancer cases are expected to be diagnosed (Table 1). Lung cancer is projected to remain the most diagnosed cancer in Canada, with 32 100 new cases expected in 2024. Breast (30 800 cases), prostate (27 900 cases) and colorectal (25 200 cases) cancers are expected to be the next most common cancers. Combined, these 4 cancer types are 47% of all new cancer cases expected in 2024.
Projected estimates of new cases and age-standardized incidence rates (ASIRs) for cancers in Canada, by sex, 2024
Among males, the most commonly diagnosed cancers are expected to be prostate (22%), lung (12%), colorectal (11%), and bladder (7%) cancers. Among females, breast (25%), lung (14%), colorectal (9%), and uterine (7%) cancers are expected to be the most commonly diagnosed cancers. Apart from sex-specific cancers, cancer is more commonly diagnosed among males than females, except for breast, thyroid, and lung cancers, which are more common among females (Table 1). Overall, the age-standardized incidence rate (ASIR) for all cancers combined is expected to be 13% higher among males than females (562.2 v. 495.9 per 100 000) in 2024.
Mortality in 2024
In 2024, 88 100 people in Canada are expected to die of cancer (Table 2). Lung cancer is expected to remain the most common cause of cancer death, with an expected 20 700 deaths in 2024. These deaths will account for almost one-quarter of all cancer deaths in Canada. Colorectal (9400 deaths), pancreas (6100 deaths), breast (5500 deaths), and prostate (5000 deaths) are projected to be the next most common causes of cancer death. Combined, these 5 cancers are expected to account for more than half (53%) of all cancer deaths in Canada in 2024.
Projected estimates of deaths and age-standardized mortality rates (ASMRs) for cancers by sex, Canada, 2024
For both males and females, lung cancer accounts for the highest number and proportion of cancer deaths at 10 900 (23%) and 9800 (24%) projected deaths, respectively. Colorectal (11%), prostate (11%), pancreas (7%), and liver and intrahepatic bile duct (5%) cancers are the next most common causes of cancer death among males, while among females, the next leading causes of cancer death are breast (13%), colorectal (10%), pancreas (7%), and ovarian (5%) cancers.
The age-standardized mortality rate (ASMR) is expected to be markedly higher (37% higher) among males than females (209.6 v. 152.8 per 100 000, respectively) in 2024. Apart from sex-specific cancers, males are expected to have higher mortality for all cancer types except for breast cancer (Table 2).
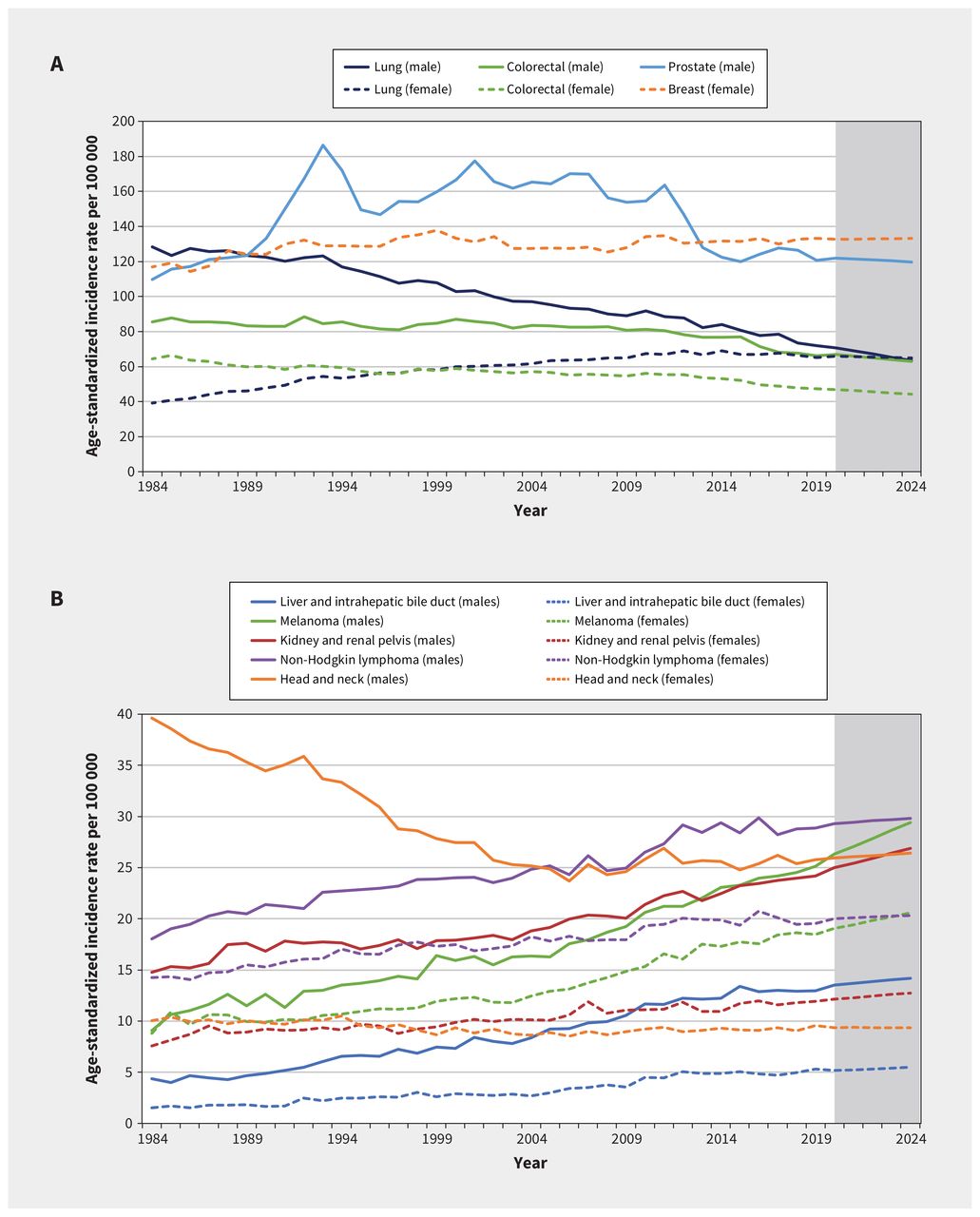
Incidence over time
The trends in ASIR for the most common cancer types for both males and females are presented in Figure 1. Over the study period, ASIRs for all cancers combined and the most common cancer types have been higher among males than females. Notably, however, incidence rates of lung cancer have converged for males and females, with females expected to have slightly higher incidence of lung cancer in 2024. Incidence rates of colorectal cancer have been declining in recent years for both males and females. In 2024, the incidence of colorectal cancer is expected to be 26% and 31% lower than in 1984 among males and females, respectively.
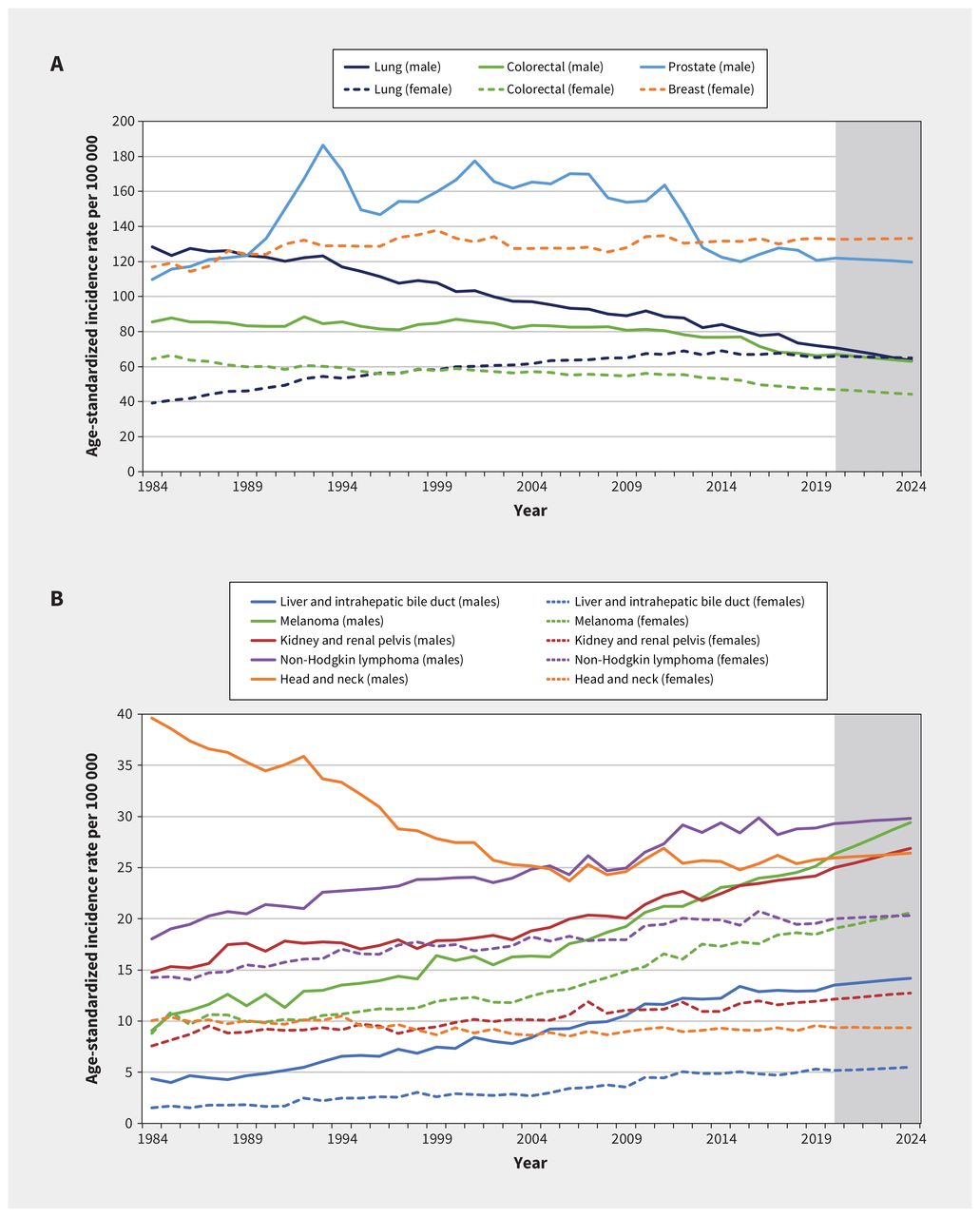
Age-standardized incidence rates for (A) the most common cancers (lung, colorectal, prostate, breast) and (B) additional cancers (liver and hepatic bile duct, melanoma, kidney and renal pelvis, non-Hodgkin lymphoma, head and neck) in Canada, by sex, 1984–2024. Data from 1984 to 1991 were from the National Cancer Incidence Reporting System and data from 1992 to 2019 were from the Canadian Cancer Registry. Analyses were conducted by Statistics Canada at the Centre for Population Health Data. Projected data for 2020–2024 are shown in shaded areas.
Mortality over time
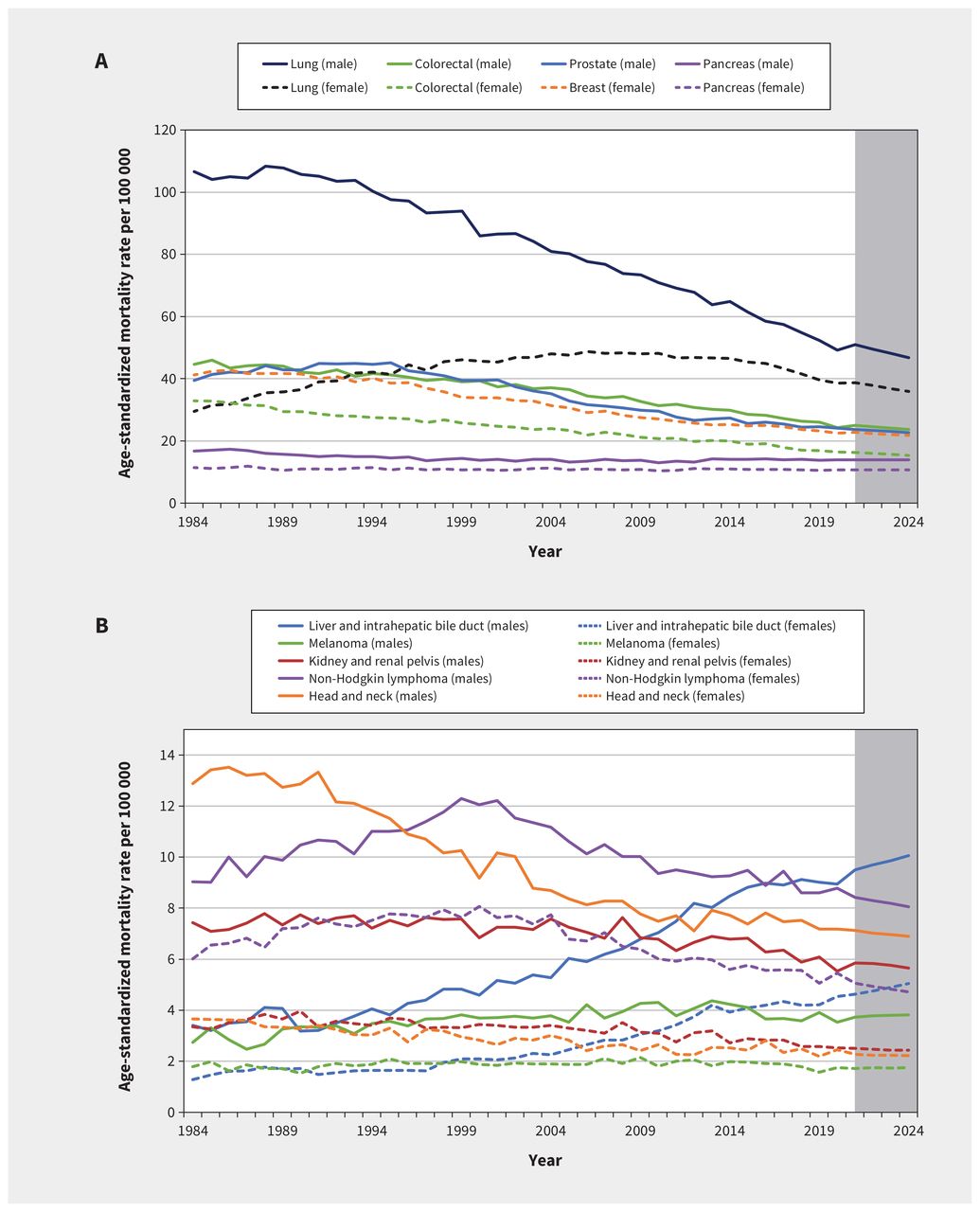
The trends in ASMR for the most common causes of cancer death for both males and females are presented in Figure 2. For all cancers combined and the most common causes of cancer death, ASMRs have been higher among males than females over time. Mortality from lung cancer has been declining among males since its peak in 1988, with steady decline thereafter. For females, this peak occurred in 2006 and the rate has since declined.
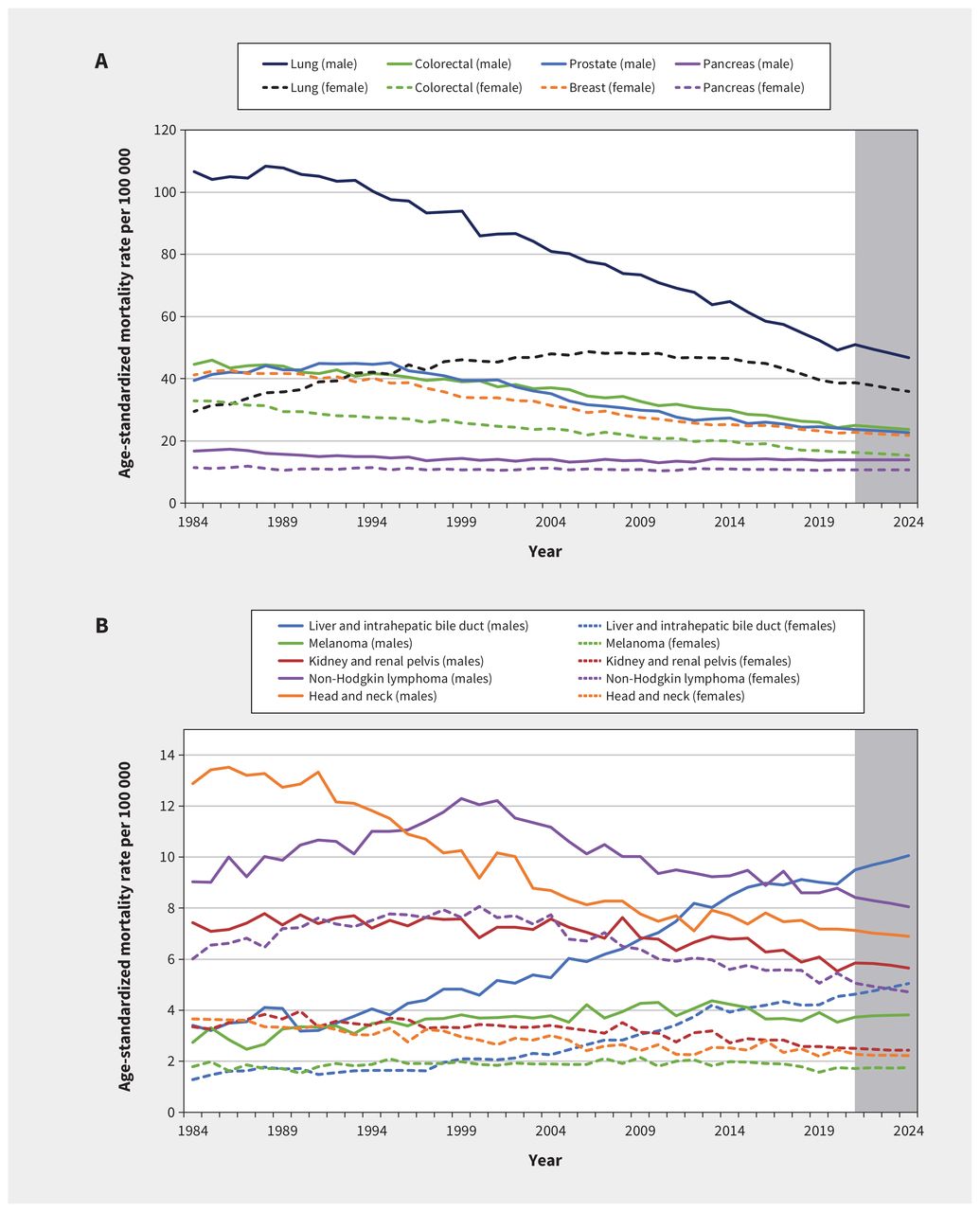
Age-standardized mortality rates for (A) the most common cancers (lung, colorectal, prostate, breast, pancreas) and (B) additional cancers (liver and hepatic bile duct, melanoma, kidney and renal pelvis, non-Hodgkin lymphoma, head and neck), in Canada, by sex, 1984–2024. Data from 1984 to 2020 were from the Canadian Vital Statistics Death Database. Analyses were conducted by Statistics Canada at the Centre for Population Health Data. Projected data for 2020–2024 are shown in shaded areas.
Notable trends outside of most common cancers
Over time, incidence and mortality for liver and intrahepatic bile duct cancers have been increasing among both males and females (Figure 1B and Figure 2B). Incidence of kidney and renal pelvis cancer has also been increasing, particularly among males, although mortality has decreased in recent years. Incidence of melanoma continues to increase for both males and females, although mortality has remained largely stable. Although relatively stable among females, incidence of head and neck cancer among males decreased considerably from 1984 to 2005, and has been rising since. Mortality from head and neck cancer has decreased among males and females.
Non-Hodgkin lymphoma is expected to be the fifth most diagnosed cancer, accounting for 5% of new cancers among males and 4% among females. Incidence of non-Hodgkin lymphoma increased until the mid-2010s, more among males than females (Figure 1B). Conversely, mortality has been declining for this cancer type over the last 2 decades for both sexes (Figure 2B).
Incidence and mortality across Canada
Projected ASIRs and counts of new cancer cases for 2024 are provided by cancer type and region in Appendix 2, Supplementary Table 2 and Table 3, respectively, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.240095/tab-related-content; ASMRs and cancer deaths in 2024 are provided in Appendix 2, Supplementary Table 4 and Table 5, respectively. Both ASIRs and ASMRs showed considerable variability across geographic regions. For all cancers combined, ASIRs are generally higher in eastern Canada (Appendix 3, Supplementary Figure 1A, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.240095/tab-related-content).
Projected ASMRs are generally lower in western Canada (Appendix 3, Supplementary Figure 1B). We also observed notable differences in projected ASIRs and ASMRs for specific cancer types across provinces and territories, as shown in Appendix 2, Supplementary Table 2 and Table 4. For the most part, overall ASIRs are higher in the Atlantic and eastern provinces than in western provinces, driven by differences in common cancers such as lung, colorectal, and breast cancer.
Interpretation
Although the number of cancer cases in 2024 is expected to rise compared with previous years, overall cancer incidence and mortality continue to decline. These declines are likely owing to continued efforts across the cancer control spectrum and improvements in prevention, screening, and treatment, particularly for certain cancers where concerted efforts have occurred.19
The overall survival among people with cancer continues to improve,20–22 contributing to a growing number of people living with and beyond cancer. Our estimates in 2022 suggested that more than 1.5 million people in Canada were living with and beyond cancer up to 25 years after diagnosis.23 This growing population of cancer survivors, combined with the projected annual increase in the total number of new primary cancers in 2024, will have a substantial impact on Canadian health care systems, given ongoing needs of people with a history of cancer. The increase in the number of cancer survivors will require both additional investment and innovation to provide necessary supports.24
Cancer remains the leading cause of death in Canada. Estimates from the Centre for Population Health Data at Statistics Canada, released in 2023, suggest that cancer accounted for nearly 25% of all deaths in Canada in 2022.25 In terms of potential years of life lost before age 75 years, the impact of cancer is even more profound. Between 2018 and 2020, more than 1 322 000 potential years of life were lost from cancer. These data suggest that cancer is also by far the leading cause of premature death in Canada.3
Notable improvements continue in terms of lung and colorectal cancer incidence and mortality. The impact of tobacco cessation and avoidance on incidence of lung cancer continues to be observed.26,27 However, among females, reductions in lung cancer incidence have not been as pronounced, and more cases are expected to be diagnosed among females than males in 2024 in Canada. In the United States, higher rates of lung cancer have been observed among younger women, which may not be fully explained by tobacco consumption patterns.28 For colorectal cancer incidence, organized screening programs have led to large reductions in ASIRs in recent years.29,30 For both lung and colorectal cancers, improvements in diagnostic pathways and clinical management have led to reductions in mortality, with improved survival reported for most stages at diagnosis.20,31–33
In our analyses, we highlighted several other cancers (i.e., liver and intrahepatic bile duct cancer, kidney cancer, melanoma and head and neck cancers) with concerning trends. Over the past 4 decades, some of the fastest increases in cancer rates in Canada were seen for these cancers. Increases in incidence of liver and intrahepatic bile duct cancers have been tied to factors such as alcohol consumption,34 hepatitis B and C infection,35 excess body size,36 and diabetes.37 Kidney cancer has emerged as one of the cancers most strongly associated with excess body size,36 diabetes, 38 and high blood pressure.39 The rise in melanoma is a continued cause for concern, given the known relationship with exposure to ultraviolet radiation; continued investment is required for preventive personal and policy efforts.40 Also included in the mid-incidence group are cancers of the head and neck. Diverse risk factors and epidemiological trends in tobacco and alcohol consumption, 41 along with human papillomavirus (HPV) infection,42 are affecting these rates and merit continued attention.
Although substantial progress has been made in reducing incidence of cervical cancer over the past decades, recent trends suggest that rates have plateaued and have even started to increase. The rate remains relatively low (7.8 cases per 100 000), but the observed recent increase is concerning given that cervical cancer is largely preventable. Similar trends have been observed in the US, with increases in late-stage diagnoses43 and overall rates among younger age groups (30–40 yr).44 A study in British Columbia from 1971 to 2017 found similar attenuation of declining rates among younger age groups (< 45 yr).45 These projections suggest that continued intervention is needed to reach the goal of eliminating cervical cancer in Canada.24 The World Health Organization suggests that countries should strive for fewer than 4 cases per 100 000 by 2030 through the widespread uptake (> 90%) of HPV vaccination programs and HPV testing as the primary screening modality.46
A major update to our analyses is the inclusion of data from Quebec, enabled by the submission of 2011–2017 incidence data to the Canadian Cancer Registry from the Quebec cancer registry. 3 Compared with previous efforts to model national data, the projected estimates from this analysis are likely more accurate for Quebec and Canada, given the inclusion of the previously missing Quebec data.
Limitations
A major limitation of currently available population-level cancer data in Canada is the lack of individual-level data on social determinants of health such as income, education, and race and ethnicity. Although provincial cancer registries are mandated to collect data to capture pathologically confirmed diagnoses of cancer, measures of social determinants are not captured by provincial or regional health authorities for inclusion in registries. Despite these limitations, data from area-level analyses of socioeconomic status and regional-specific analyses of individual-level data in Canada show the strong effects of social factors on cancer incidence and mortality.47–49 In particular, large effects have been observed for cancers for which there are organized screening programs50 or strong exposures related to social gradient such as smoking and lung cancer.51
The estimates here are projections based on the most up-to-date national cancer data and may be subject to variability over time. Because of the intensive nature of registering cancer diagnoses and deaths, data availability is delayed. Although we included 2020 mortality data from the Canadian Vital Statistics Death database, we included incidence data up to 2019 in the projections to avoid biasing projections because of pandemicrelated effects. Reports have suggested that decreases in diagnoses of cancer observed in 2020 were related to pandemic responses.52,53 These changes are more a reflection of differences in practice patterns during the pandemic than actual changes in the underlying incidence, which may bias short-term projections away from the actual trends in cancer incidence. Subsequent iterations of our analyses will inform projections of trends less affected by service interruptions or altered diagnostic patterns from the pandemic response.
We did not include data from Quebec (2018, 2019) and Nova Scotia (2019) because of reporting delays. These differences are likely to have minimal impact on the overall projections of national data. Furthermore, although the CANPROJ approach has been validated using Canadian data, specific validations for each province have not been performed. In addition, changes to cancer site definitions have occurred during the data years included in the projections (Appendix 1). These are likely to have minimal impact on the reported trends since the current definitions were retroactively applied to all diagnosis years used for projection purposes and are in alignment with changes in definitions for other national cancer registries (e.g., the North American Association of Central Cancer Registries).
Conclusion
These estimates highlight the substantial impact of cancer on people and health systems in Canada. Although the continued reduction in ASIRs and ASMRs that we project reflect increased survivorship and lower cancer incidence related to considerable efforts in prevention, screening, and treatment, continued investment across all areas of cancer control and care are needed to reduce the impact on all people affected by cancer in Canada.
Footnotes
Competing interests: Darren Brenner reports support from the Canadian Cancer Society and the Canadian Partnership Against Cancer. Ryan Woods reports funding from the BC Cancer Foundation, the Canadian Partnership Against Cancer, and Statistics Canada. Donna Turner reports support to attend meetings from the Canadian Cancer Society. No other competing interests were declared.
This article has been peer reviewed.
Contributors: All of the authors contributed to the conception and design of the work, and the acquisition, analysis, and interpretation of data. All of the authors drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding: This study was developed by the Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada, and the Public Health Agency of Canada and was therefore supported by public and donor funding. No external sources of funding were obtained for this study.
Data sharing: The data included in these analyses are available to the public and researchers through application and access from the Research Data Centres of Statistics Canada.
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Canadian Cancer Society.
- Accepted March 28, 2024.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections